Sinus Lift in Implant Dentistry: Lateral Window or Transcrestal Approach?

Table of Contents
Related clinical guides
A sinus lift is a planning decision, not just a grafting technique
Whenever I plan an implant in the posterior maxilla, I remind myself that this is the most honest region in the mouth. The bone tells you the truth. It does not pretend to be denser than it is, and the maxillary sinus floor sits there, quietly, deciding how much ambition I am allowed to have. A sinus lift is the procedure we reach for when that floor sits too close to the crest to place an implant of useful length. But here is the framing I want you to leave with: a sinus lift is a planning decision before it is ever a surgical one. The day I started treating it as a decision tree instead of a single technique, my cases got calmer and my complications got rarer.
This article is written for clinicians. I will keep my own uncertainty visible, because the literature on sinus floor augmentation is large, occasionally contradictory, and easy to oversell. I want you to finish reading with a clearer sense of when to elevate, how to elevate, and (this matters most) when not to elevate at all.
The short answer, before the detail
For smaller vertical gains in a healthy sinus, a transcrestal approach is usually enough. For larger gains, anatomically complex sinuses, or staged reconstructions, a lateral window gives you control and visibility. Neither is "better." They solve different problems, and the residual bone, the membrane, and the anatomy choose for you.
Hold that thought lightly. By the end I will have complicated it on purpose, because the cleanest-sounding rule in implant dentistry (residual bone height decides everything) is the one that has aged the worst.
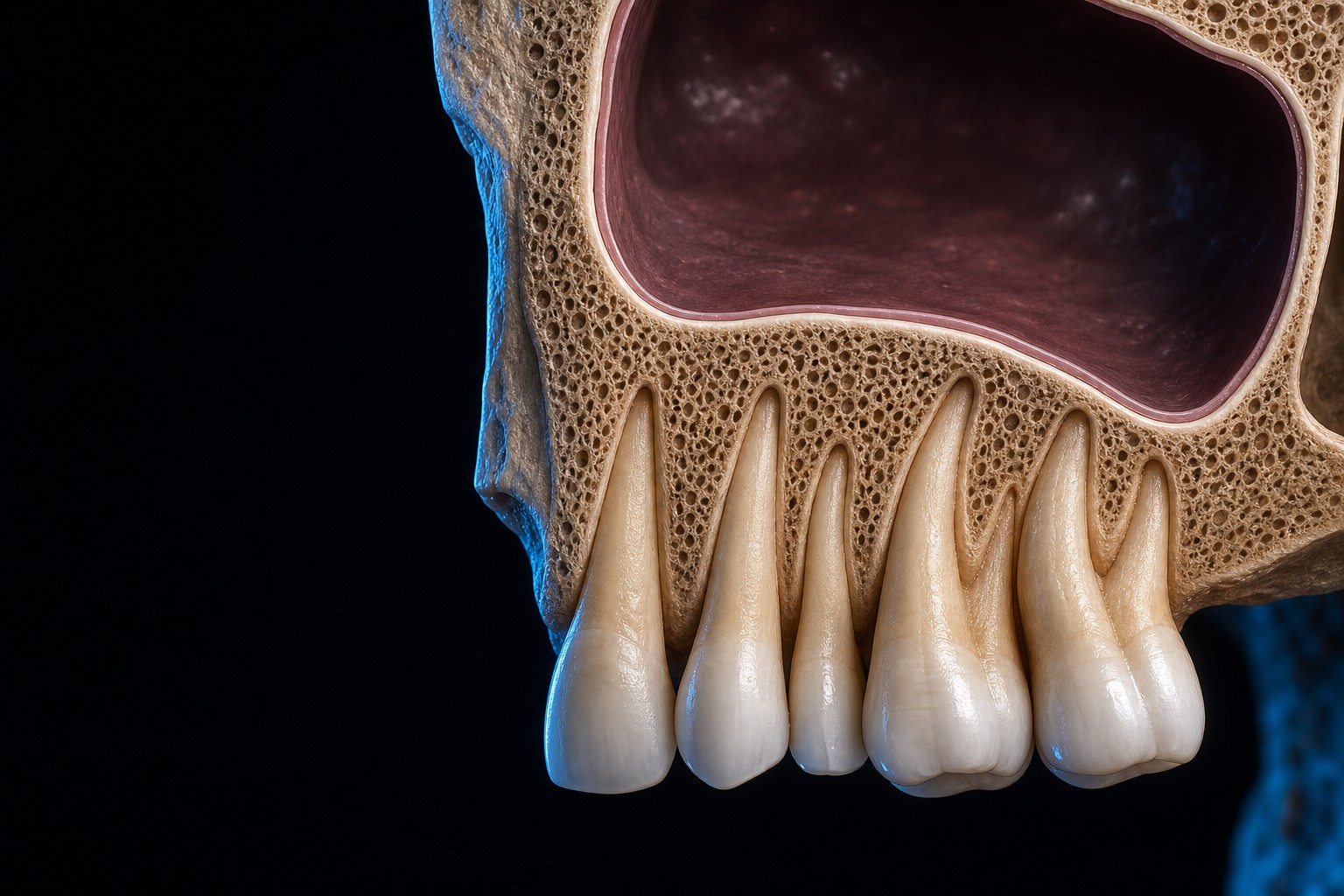
What a sinus lift is trying to solve
After we lose posterior maxillary teeth, two things happen at once. The alveolar ridge resorbs from above, and the sinus pneumatizes from below. The air space expands into the space the roots used to occupy. The result is a thin shelf of bone between the crest and the sinus floor, often too thin to anchor an implant of useful length.
A sinus lift solves this by elevating the Schneiderian membrane (the thin mucosal lining of the sinus floor) away from the bone, then placing graft material, a blood clot, or simply the implant itself into the protected compartment that elevation creates. New bone forms in that compartment. That is the whole idea: create a contained, vascularized space under an intact membrane and let it ossify.
The word "intact" is doing heavy lifting in that sentence. Almost everything that goes wrong in sinus surgery traces back to the membrane, the anatomy around it, or a decision made before the flap was ever raised. So let us start where the planning starts.
Maxillary sinus anatomy you actually use during a sinus lift
You do not need to recite anatomy to lift a sinus. You need to read a CBCT and predict where the trouble lives. Four structures decide most of your cases.
The Schneiderian membrane
A healthy Schneiderian membrane is roughly 0.5 to 1 mm thick on imaging (histologic sections put it thinner, around 0.13 to 0.5 mm). Mucosal thickening greater than 2 mm is extremely common, seen in roughly 36 to 60% of sinuses, and on its own it is usually not pathologic. I do not cancel a case because a CBCT shows a thickened floor lining.
Here is the counterintuitive part that changed how I handle membranes. Thicker is not automatically safer. Very thin membranes (under 0.5 mm) tear more easily, and the relatively forgiving window sits around 1.5 to 2 mm. Membranes thicker than 3 mm, on the other hand, carry more risk and can signal underlying pathology that deserves attention before I touch anything.
Antral (Underwood) septa
Bony septa cross the sinus floor in roughly a third of sinuses. They matter enormously because they sharply raise the perforation risk: a 2024 systematic review found membrane perforation in about 39.8% of sinuses with septa versus about 12.3% without, an odds ratio near four (Yang et al., PLOS One 2024). When I see a septum on CBCT, I plan my window around it, sometimes as two smaller windows, and I slow down. A septum is the single most common reason a routine lateral window stops feeling routine.
The posterior superior alveolar artery
The PSAA runs in the lateral sinus wall, usually intraosseous. Across cone-beam CT anatomy studies it sits roughly 7 mm above the sinus floor and about 15 mm above the crest. Here is the humbling fact: even with modern high-resolution CBCT it is reliably visualized in roughly 70 to 90% of cases, so a meaningful minority of the time you are operating where you cannot see it. When the vessel is visible and its diameter exceeds 2 mm, bleeding risk during the window osteotomy rises, and I adjust my osteotomy height to stay clear of it.
The ostium and muco-ciliary drainage
The sinus drains through an ostium that sits high on the medial wall. The muco-ciliary system sweeps mucus toward it, and that drainage has to stay patent. This is the structure people forget. If you over-graft, or if pre-existing thickening already crowds the upper sinus, you can obstruct the ostium and turn a clean graft into a sinusitis. Lift what you need, not more.
Residual bone height: a ladder, then a correction
Most of us were taught a clean threshold ladder for residual bone height, and the decision tree from Lyu and colleagues (2023) is a good, current version of it.
| Residual bone height | Default approach | Notes |
|---|---|---|
| Greater than 6 mm | Transcrestal | Comfortable territory for crestal elevation |
| 4 to 6 mm | Transcrestal if the sinus and membrane are healthy; lateral if not | Membrane status tips the decision |
| 2 to 4 mm | Lateral if the lateral wall is under 2 mm thick; otherwise transcrestal | Wall thickness tips the decision |
| Under 2 mm | Individualized | No reflex answer; plan case by case |
That ladder is genuinely useful. Use it. But here is the correction I want every reader to internalize, because it is where modern practice has moved.
Residual bone height is a guide, not a gate. The real driver of whether you can place an implant at the same time as the lift is not the millimeters on the scan, it is the primary stability you can actually achieve. Predictable simultaneous placement has been reported even at 1 to 2 mm of residual height when the clinician could obtain stability. So the scan starts the conversation; the torque wrench and your tactile sense finish it. If I cannot get stability, I stage. If I can, the residual height number stops being a veto.
Crestal versus lateral window: the framing that matters
| Dimension | Transcrestal (crestal) | Lateral window |
|---|---|---|
| Typical indication | Smaller vertical gains, healthy sinus | Larger gains, complex anatomy, staged cases |
| Visibility | Blind or semi-blind | Direct visual access to the membrane |
| Membrane control | Limited, tactile | High, you can see and manage tears |
| Morbidity | Lower | Higher |
| Handling septa or a low artery | Poor | Good |
| Graft volume | Modest | Large |
The table is a starting grid, not a verdict. The honest version is: choose the least invasive approach that still gives you control over the membrane and the anatomy you saw on the CBCT.
Transcrestal sinus floor elevation
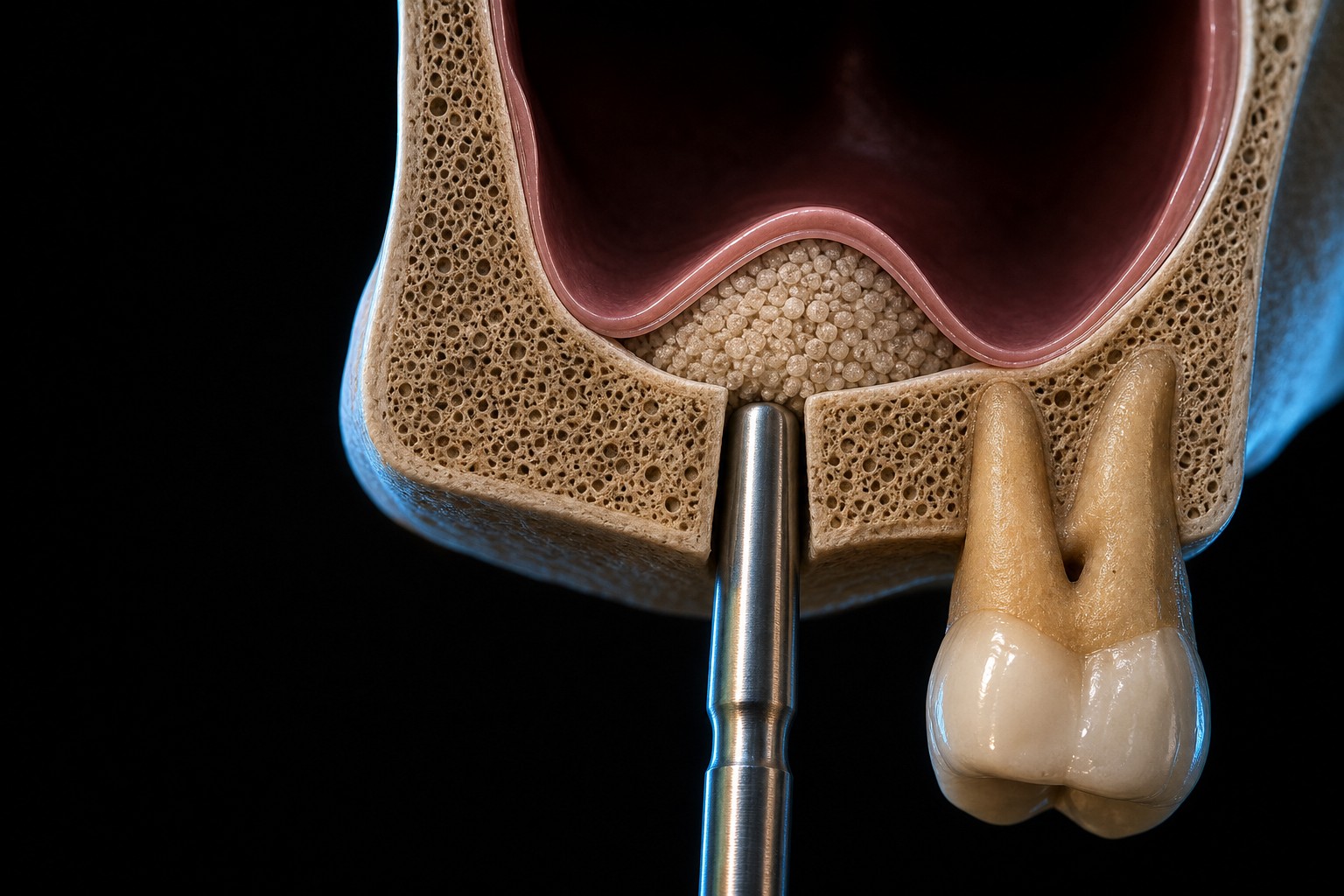
The transcrestal approach works through the implant osteotomy itself. You prepare up to the floor, then elevate the membrane through that small access, with osteotomes, hydraulic pressure, or dedicated reamers, and place graft or just the implant.
Two myths deserve to die here. The first is the old "you gain about 1 mm of bone for every mm you push" linear story. Bone gain is non-linear and generally modest, particularly when you elevate without graft and rely on the clot. Promise modest gains, not millimeters-on-demand. The second myth is that crestal means tear-free. Perforations are less frequent here than in lateral windows, but they are real, and thin membranes are the usual culprit. You just cannot see them as well, which is exactly why I keep crestal elevation for the smaller, healthier sinuses.
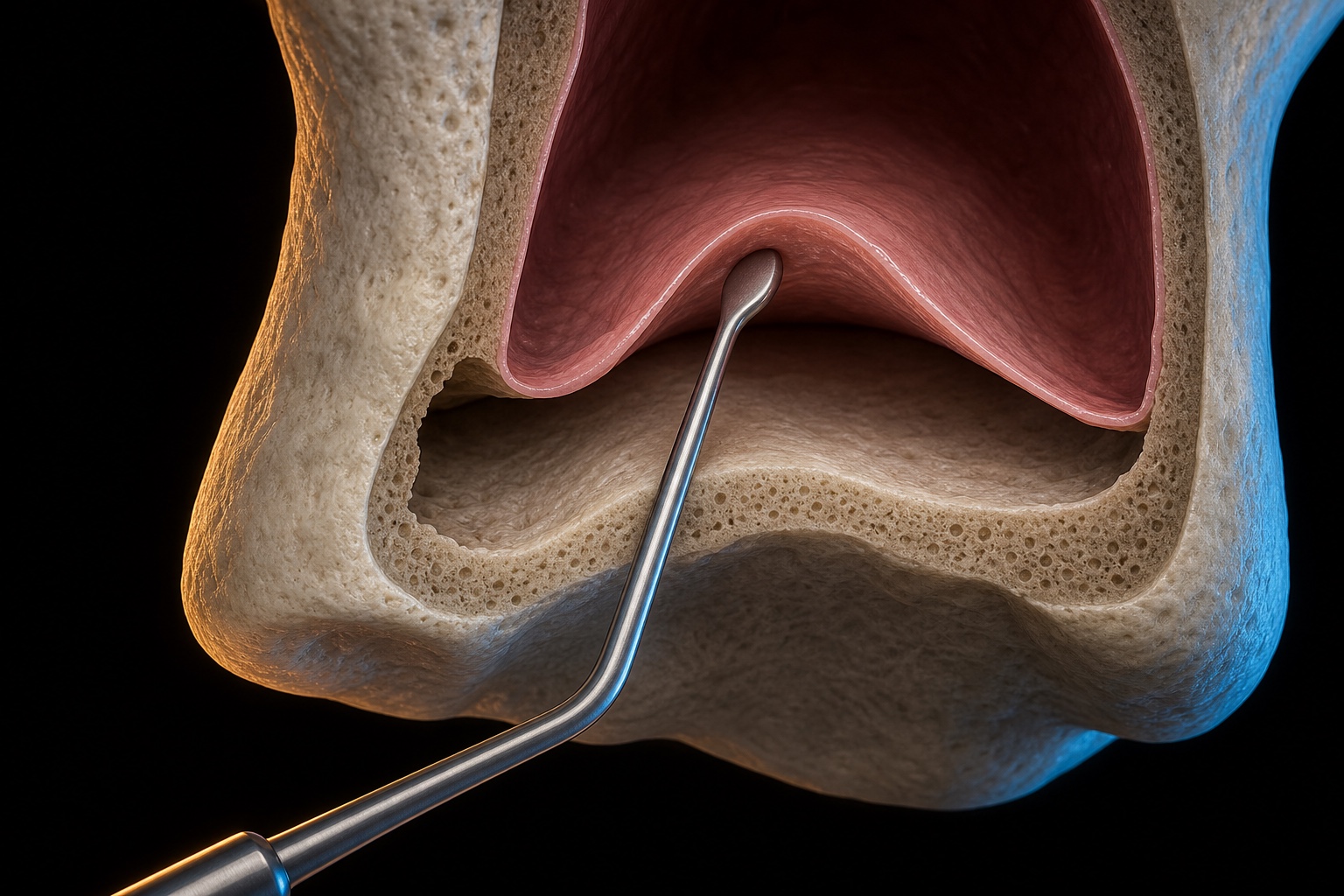
Lateral window sinus lift
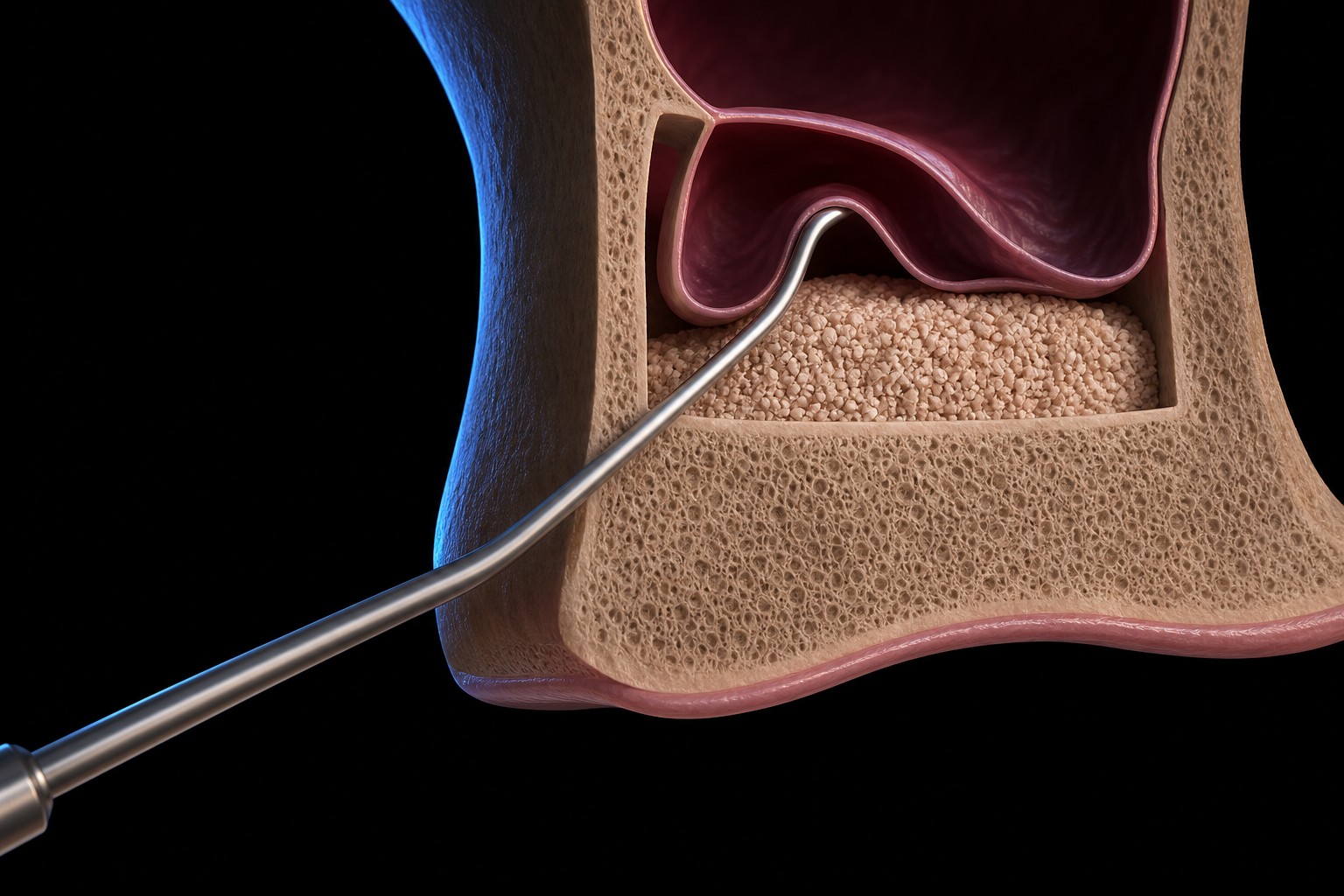
The lateral window trades morbidity for control. You open a window in the lateral wall, see the membrane directly, elevate it under vision, and graft a compartment you can actually measure. This is the approach for larger gains, for septa, for a low or large artery, and for staged reconstructions where you want maturation before you commit an implant.
A practical detail with evidence behind it: covering the lateral window with a barrier membrane and using rough-surface implants is associated with better outcomes (more on the survival numbers below). The window is also where you earn your understanding of perforation management, because here you will both cause and fix tears under direct vision.
Graft materials: survival is similar, behavior differs
This is where I have changed my mind the most over the years. We argue about graft material as if it decides implant survival. The data say it largely does not.
In Del Fabbro's analysis, overall implant survival in grafted sinuses was about 91.5%. Broken down by material: autogenous bone alone around 87.7%, autogenous plus a substitute around 94.9%, and substitute alone around 96.0%. Read that again. Substitutes performed at least as well as autogenous bone. The material you pick is not the lever that moves survival.
| Material | Implant survival signal | Graft behavior |
|---|---|---|
| Autogenous alone | ~87.7% | Resorbs substantially over time |
| Autogenous + substitute | ~94.9% | Intermediate |
| Substitute alone | ~96.0% | Stable |
| Xenograft (DBBM) | Within the substitute range | Resorbs slowly, best space maintenance |
What does differ is behavior. Autogenous bone resorbs substantially, often cited near or above 40% volume loss, so the volume you packed is not the volume you keep. Deproteinized bovine bone mineral (DBBM, a xenograft) resorbs slowly and holds space best, though reported 6-month resorption varies across studies, so treat any single percentage as approximate rather than settled. That is why so many of us reach for a xenograft or a xenograft blend when volume stability over time is the priority.
The graftless option
You can also elevate the membrane, place the implant to tent the space, and let the blood clot alone ossify around it, no particulate graft. Graftless lateral window cases report implant survival around 97.9 to 98.3%, which is excellent. The trade-off is honest: less vertical bone gain (about 1.73 mm less) and lower density of the new bone. So graftless is a real option when you need less height and have good stability, and a poor option when you need maximal volume.
Platelet concentrates
L-PRF and similar platelet concentrates are reasonable adjuncts. The certainty around them is low, and they are not a survival driver. I use them as handling and biologic helpers, not as the thing I expect to change the outcome.
Simultaneous versus staged placement
The decision to place now or place later follows from one question, and it is not "how many millimeters of bone are on the scan." It is "can I achieve primary stability today?"
- If you can achieve stability, place the implant simultaneously with the lift. The same primary-stability logic that governs immediate implant placement applies here: stability, not the millimeters on the scan, decides whether you place now.
- If you cannot, stage it. Graft now, let it mature, and place later.
When you stage, plan for roughly 6 to 9 months of graft maturation before you place into it. Residual height influences your odds of getting stability, which is why low residual height correlates with staging, but the correlation is downstream of stability, not the rule itself. Keep your eye on the real variable.
A short note on healing and maturation
Across approaches, I plan for about 6 to 9 months before loading or second-stage surgery. One nuance worth holding: xenograft matures more slowly than autogenous bone. So when I have grafted with DBBM and I am tempted to load early, I remind myself that the slow-resorbing material that gave me beautiful volume stability is also the one asking me for patience. Match your timeline to your material.
Membrane perforation is not a footnote
Perforation is the complication everyone fears and the one most worth understanding precisely. In lateral window surgery, pooled perforation incidence commonly sits in the 20 to 30% range; the cited Diaz-Olivares review of lateral-approach cases reported a mean near 30.6% across a wide spread (roughly 7 to 60%). Transcrestal rates are lower but, again, real, driven mostly by thin membranes.
Now the single most important fact in this whole article: a perforation, by itself, does not reduce implant survival. Diaz-Olivares and colleagues (2021) reported 97.68% survival in perforated cases versus 98.88% in non-perforated cases, with p = 0.229, not a statistically significant difference. A perforation is not a reason to abort. What matters is the size of the tear and whether you manage it well.

| Perforation size | Typical management |
|---|---|
| Under 5 mm | Fold the membrane over itself, or close with a resorbable suture |
| 5 to 10 mm | Cover with a collagen membrane (the most common scenario) |
| Over 10 mm | Laminar bone plate plus collagen; consider staging |
Several named frameworks formalize this thinking, and I want to label them honestly. These are expert technique frameworks (Level V, expert opinion), not RCT-grade evidence. They are valuable precisely because they encode experienced judgment, but you should not cite them as if they were trials.
- Vlassis and Fugazzotto (1999) classification. A foundational scheme for categorizing perforations by location and the access through which they occur.
- Testori's stabilized-collagen technique. A method for stabilizing a collagen barrier over the defect so the graft stays contained.
- The Loma Linda pouch. A technique that drapes a resorbable membrane to create a pouch that holds the graft against a perforated lining.
Learn these. Use them. Just do not over-claim their evidentiary weight.
Complications beyond perforation
Perforation gets the attention, but a few other complications deserve a place in your consent conversation and your planning.
- Sinus graft infection. Uncommon, in the low single-digit percent range, but serious. An infected graft can mean losing the graft entirely. Risk factors include pre-existing sinusitis, an obstructed ostium, perforation, and contamination.
- Postoperative sinusitis. Reported in the low single digits. The same risk factors apply. This is the clinical reason the ostium and drainage matter so much: protect drainage and you protect against sinusitis.
- Benign paroxysmal positional vertigo (BPPV). This one surprises clinicians. Malleting with osteotomes can displace otoliths in the inner ear (the percussion of the mallet plus neck hyperextension on the chair), producing positional vertigo after surgery. It is usually self-limited and resolves within about a month. You reduce the risk with a gentle, more manual elevation technique and by minimizing aggressive malleting. (Testori 2023.)
Contraindications: treat the sinus before you graft it
Some sinuses should not be lifted, at least not yet. The absolute contraindications are clear:
- Uncontrolled acute or chronic sinusitis
- Ostium obstruction
- Untreated odontogenic sinus pathology
- Sinonasal tumors
The relative contraindications ask for judgment and, often, for management before surgery:
- Heavy smoking
- Uncontrolled diabetes
- Antiresorptive therapy
- Prior sinus surgery
My rule is simple: treat sinus disease before you graft. If a patient has active or odontogenic sinus pathology, that is an ENT and source-control conversation first, not a grafting conversation. Lifting into an inflamed, poorly draining sinus is how a routine case becomes a referral letter you did not want to write.
Postoperative care
Most of the postoperative protocol is about not raising sinus pressure while the membrane and graft settle. Standard expert guidance:
- Avoid nose-blowing.
- Sneeze with the mouth open.
- Avoid straws, diving, and air-travel pressure changes in the short term.
- Use saline and decongestants as indicated.
- Take antibiotics and analgesia per your protocol.
- Warn the patient that a minor nosebleed can happen, so it does not frighten them.
None of this is exotic. It is the difference between a quiet healing course and a panicked phone call.
What the survival numbers actually say
Let us quantify outcomes for both approaches, because the headline is reassuring and you should be able to quote it.
| Approach | Implant survival | Source |
|---|---|---|
| Lateral window | ~90.1% at 3 years | Pjetursson 2008 (12,020 implants) |
| Transcrestal | ~92.8% at 3 years; annual failure ~2.48% | Tan 2008 |
One caveat before anyone reads the transcrestal number as beating the lateral one: these figures come from two separate systematic reviews of different patient populations, not a head-to-head trial. Transcrestal cases self-select for healthier, lower-difficulty sinuses, so the numbers should not be read as "crestal beats lateral." They describe different case mixes solving different problems.
For the lateral window, outcomes were better with rough-surface implants and with a barrier membrane placed over the window. That is a concrete, do-this-tomorrow finding, not a vague trend. Both approaches, done well, land in survival ranges that compare favorably with implants in native bone elsewhere in the mouth. Survival, of course, is not the same as long-term health: a grafted-sinus implant still depends on the same maintenance and tissue stability that protect against peri-implantitis anywhere else. The sinus lift is, by any fair reading, a predictable procedure. The variance lives in case selection and execution, not in some inherent fragility of the technique.
Take this further
If you want the bone-side decisions behind every sinus graft worked through in one structured place, the interactive Guided Bone Regeneration ebook walks through membranes, graft materials, and space maintenance as a continuous CE module rather than a scattered reading list. It is the companion resource I point clinicians to when they want to consolidate the augmentation principles this article only touches.
Honest truth
The honest truth is that the sinus lift is more reliable than its reputation and more demanding than its marketing. The survival numbers are excellent across materials, approaches, and even across a perforation. But that reliability is borrowed against good decisions made before the flap: reading the membrane and the septa and the artery, protecting the ostium, choosing crestal versus lateral for the right reasons, and being honest about whether you can get stability today.
And the most honest line of all: sometimes the best sinus lift is no sinus lift. A tilted implant, a shorter implant, a zygomatic referral, or simply a different prosthetic plan can serve the patient better than a graft they did not need. The skill is not in performing the procedure flawlessly. It is in knowing, before you start, whether this particular patient should have it at all.
Key references
- Lyu M, Xu D, Zhang X, Yuan Q. Maxillary sinus floor augmentation: a review of current evidence on anatomical factors and a decision tree. Int J Oral Sci. 2023;15:41. doi:10.1038/s41368-023-00248-x. PMC10504247
- Pjetursson BE, et al. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part I: lateral approach. PMID 18724852
- Tan WC, et al. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part II: transalveolar technique. PMID 18724853
- Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent. 2004;24(6):565-577. PMID 15626319
- Diaz-Olivares LA, et al. Management of Schneiderian membrane perforations during maxillary sinus floor augmentation with lateral approach. Int J Implant Dent. 2021. doi:10.1186/s40729-021-00346-7. PMC8273047
- Vlassis JM, Fugazzotto PA. A classification system for sinus membrane perforations during augmentation procedures with options for repair. PMID 10397526
- Testori T, et al. Maxillary sinus elevation: clinical and complication management. Periodontol 2000. 2023. Wiley
- ITI Clinical Insights: Sinus floor elevation, overview. International Team for Implantology.
- ITI Clinical Insights: Lateral window sinus floor elevation. International Team for Implantology.
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
Peri-implantitis Treatment: Diagnose the Defect Before You Treat the Implant
Next
When the Connective Tissue Graft Was Too Good