Immediate Implant Placement: A Protocol for Case Selection and Predictable Results

Table of Contents
Related clinical guides
The most dangerous word in immediate implant placement is not immediate. It is predictable.
Immediate placement sounds efficient: extract, place, reduce appointments, keep the patient happy. In the right case it is a beautiful workflow. In the wrong case it is a fast way to create a long-term esthetic problem.
The decision is not made when the tooth is already out and everyone is looking at the socket. It is made before extraction, with the CBCT, the periapical radiograph, the soft tissue, the infection status, and the prosthetic plan in front of you.
So I do not ask whether I can place today. I ask whether I can place today without letting the socket choose the implant position.
Video: sagittal socket classification before immediate placement.
Read the sagittal root position, facial wall, and restorative axis before deciding whether immediate placement is reasonable.
Immediate Implant Placement Protocol And Case Selection
Immediate implant placement is not a single protocol. The decision starts with case selection: socket-wall integrity, facial plate thickness, infection control, primary stability, implant position, jumping distance, and whether grafting is needed to support the contour.
The International Team for Implantology defines immediate placement as placement into the socket on the same day as extraction, also called Type 1 placement (ITI implant placement and loading protocols). Their post-extraction consensus makes the core point for this article: ridge modeling continues after extraction, and augmentation can help compensate for that modeling when the case is selected correctly (ITI post-extraction consensus).
What Immediate Actually Means
Immediate placement means the implant is placed into the socket at the same appointment as extraction. It does not mean immediate loading, immediate provisionalization, or skipping grafting, and it definitely does not mean every extracted tooth deserves an implant today.
ITI consensus statements describe immediate placement as Type 1 and emphasize both its advantages and its risks: shorter treatment time and favorable contained defects in selected cases, but also higher technical difficulty, recession risk, and unpredictable post-extraction modeling ITI Consensus: Implants in Postextraction Sites.

The Four Conditions I Want Before Saying Yes
- Controlled infection. Acute uncontrolled infection changes the plan.
- A socket that allows ideal 3D position. The implant must be restorative-driven, not socket-driven.
- Primary stability. Usually apical and palatal/lingual bone, not the fragile buccal plate.
- A soft-tissue and gap plan. The buccal gap, facial wall, tissue phenotype, and provisional all need a plan.
If one of these is missing, I become much less enthusiastic.
The Buccal Wall Is The Gatekeeper
The facial plate is thin, fragile, and partly bundle bone around many anterior teeth. Bundle bone is tooth-dependent: it is supplied by vessels that run inside the periodontal ligament, so the moment the tooth leaves the socket, part of the buccal wall loses its blood supply and begins to resorb. Placing an implant the same day does not stop this. The implant osseointegrates with the bone that survives, but it cannot rescue a wall that has lost its biological reason to exist. The ITI consensus is explicit that ridge modeling continues after extraction and that immediate placement carries recession risk, especially with thin tissue, thin facial bone, dehiscence, or malposition ITI Consensus: Implants in Postextraction Sites.
That is why the buccal wall is not just another wall. It is the wall the patient will see later. A small midfacial recession on a palatal surface is invisible; the same recession on the buccal of a maxillary central incisor is the difference between a result the patient shows off and one the patient hides.
Before I commit, I want three answers from the CBCT and clinical exam. Is the buccal plate intact along its full height, or is a fenestration or dehiscence hiding under healthy-looking gingiva? How thick is it, since a thick-wall phenotype tolerates immediate placement far better than a thin, scalloped one? And where does the soft-tissue margin sit relative to the adjacent teeth, because tissue that is already slightly receded has almost no reserve to give.
If the buccal wall is absent, fenestrated, or too thin to support the esthetic plan, I do not try to be heroic. I consider early placement after soft-tissue healing, alveolar ridge preservation, or a staged approach with guided bone regeneration to rebuild the wall first. When the wall is compromised, the more controlled path is almost always to rebuild and place into healed, predictable bone.
The Jumping Distance And The Buccal Gap
The jumping distance is the horizontal gap between the implant surface and the inner aspect of the socket wall. In immediate placement, the implant is deliberately positioned toward the palatal or lingual wall to engage stable bone and keep the platform away from the fragile buccal plate, which leaves a buccal gap by design.
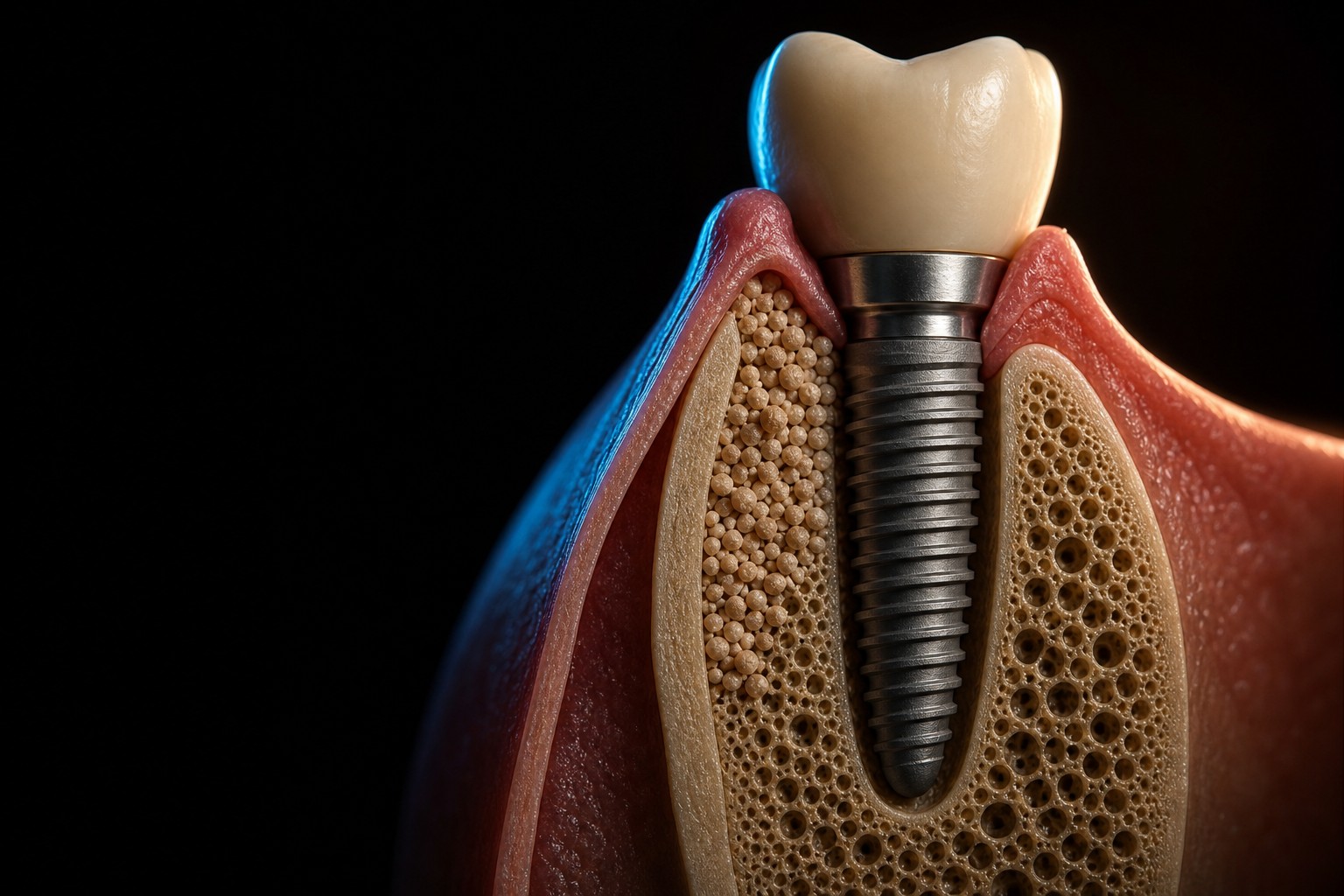
That gap is not a mistake if the implant is positioned correctly; it is the expected consequence of placing the implant in the restoratively correct position rather than the path of least resistance. The mistake is letting the gap dictate where the implant ends up. The implant should be palatal because that is where the restoration wants it, not because grafting the gap is inconvenient.
How I read and manage that gap depends on its size, the thickness of the buccal wall in front of it, and whether the wall is intact at all. A small contained gap behind a thick plate is a different problem from a wide gap behind a paper-thin wall, which is different again from a frank dehiscence where the wall is gone. My practical approach:
| Gap/defect situation | Direction |
|---|---|
| Small contained gap with thick buccal wall | Monitor or graft depending on esthetic risk and material preference |
| Moderate buccal gap in esthetic area | Fill with slow-resorbing particulate graft to support contour |
| Buccal dehiscence | Treat as a GBR defect, not a simple gap |
| Missing facial wall or poor implant position | Stage the case |
The moment the buccal wall is missing, you are no longer only doing immediate placement. You are doing defect reconstruction, and the case should be planned and consented as such. Graft particles placed into the jumping gap support the contour and compensate for the modeling the consensus tells us will happen anyway; they are not a substitute for an intact wall. When the defect is contained the biology is forgiving, but when it is not, the predictable bone-regeneration principles that govern any augmentation apply: primary wound stability, space maintenance, an undisturbed clot, and protection of the graft from micromovement, the conditions Wang and Boyapati distilled into their widely cited regeneration principles (Wang and Boyapati, 2006).
A buccal dehiscence around an immediate implant is best treated as a guided bone regeneration defect rather than a simple gap fill: it usually needs a particulate graft for volume, a barrier membrane to hold space, and a flap design that achieves tension-free primary closure. The threshold for converting from gap graft to real GBR is exactly the judgment that separates a durable result from a relapse.
Immediate Molar Implants: Different Problem, Same Discipline
Molar sockets can look generous, but they bring their own traps: septum anatomy, wide and often divergent sockets, proximity to the mandibular canal or the maxillary sinus, and real difficulty controlling implant position. The temptation is to let the septum guide the osteotomy. A tall, wide interradicular septum gives you native bone to engage and a natural landmark for the axis, but it can also drag the implant away from the prosthetic center, leaving a screw access hole through a cusp tip or an emergence profile no laboratory can rescue.
In the maxilla the additional question is vertical: a thin or pneumatized septum may not give enough bone height for primary stability without engaging the sinus floor. When the residual bone below the sinus is borderline, the honest plan may be staged augmentation rather than a heroic same-day placement, a trade-off that overlaps directly with the sinus lift decision. In the mandible the limiting structure is the canal, and the depth below a molar socket apex is frequently less than it looks on a panoramic image, one more reason the CBCT is not optional here.
Surgical video: molars are a different immediate implant problem.
Molar sockets look generous, but the real risk is position control: the septum can help you or pull the implant away from the prosthetic center.
For molars, I check:
- septum width, quality, and apical anatomy
- furcation infection or bone loss
- interradicular position versus the prosthetic center and restorative emergence profile
- whether a custom healing abutment or provisional can seal and shape the site
The unifying discipline is the same one that governs the anterior case: the implant position is decided by the future restoration and the available stable bone, not by the shape of the socket you happen to be looking at. A molar socket with no septum and no apical bone to engage is not an immediate-placement site that day. Socket grafting and a delayed implant into healed bone is not a failure of nerve; it is the version of the case you would still defend in five years.

Immediate Provisionalization Is A Separate Decision
Do not let the patient, the schedule, or social media decide the provisional. Immediate provisionalization is a powerful tool in the esthetic zone, because it lets you support the gingival architecture and shape the emergence profile while the tissue still remembers the contour of the natural tooth. But it is a separate decision from immediate placement, with its own prerequisites.
It requires genuine primary stability, an occlusal scheme that keeps the provisional out of all centric and excursive contacts, a good three-dimensional implant position, and a restoration that shapes soft tissue without loading the implant dangerously. The most useful concept here is the distinction between the critical contour, the part of the emergence profile just apical to the gingival margin that determines where the margin sits, and the subcritical contour apical to that, which supports the underlying soft tissue. A provisional overcontoured in the critical zone pushes the tissue apically and manufactures the recession you were trying to avoid; a slightly concave subcritical contour invites the tissue to fill in. If the prerequisites are not all present, use a healing abutment, a customized healing component, or a delayed provisional rather than forcing a same-day crown onto an implant that is not ready to carry it.
A common mistake is to confuse stability with the right to load. An implant can be torqued to a high insertion value and still be a poor provisional candidate, because the stability is coming from compression of thin walls that will remodel, or because the occlusion cannot be controlled. Immediate placement and immediate provisionalization are related, but they are not the same treatment.
Surgical video: provisional shape is biology, not decoration.
The provisional or custom healing component should shape tissue without creating pressure, load, or a cleansability problem.
Soft Tissue Is Part Of The Surgery, Not An Afterthought
Hard tissue keeps the implant. Soft tissue keeps the result looking like a tooth, so the soft-tissue plan has to be made at the same time as the surgical plan. A flapless approach preserves the blood supply to the buccal plate and the papillae and is often kindest in an intact, thick-walled socket, but gives less access to manage a graft or dehiscence. Raising a flap gives access and the ability to close over a graft, but disrupts the periosteal blood supply and can itself drive buccal remodeling. The choice follows the wall, the phenotype, and whether you are reconstructing a defect.
Tissue thickness is its own risk factor. A thin gingival phenotype shows the gray of the abutment or the shadow of a resorbing wall far more readily and has less resistance to recession. This is why a connective tissue graft is so often planned alongside immediate placement in the esthetic zone: adding thickness at the time of surgery buys tolerance against the modeling the consensus promises will happen.
The long-term enemy of every immediate implant is the same as for every implant: peri-implant disease. A site that is over-contoured, hard to clean, or left with a thin, mobile band of tissue will eventually inflame, so designing a cleansable emergence profile and adequate keratinized tissue is primary prevention. When inflammation does take hold, the management ladder is the one set out in the peri-implantitis treatment protocol, and the best version of that conversation is the one you never have to start.
Complications And How To Manage Them
Every immediate implant carries a short list of complications that are predictable enough that you should plan for them, not improvise once they happen.
Midfacial recession is the signature esthetic complication. It is driven by the factors the consensus names as risk indicators: a thin phenotype, a thin or breached buccal wall, a malpositioned implant that is too buccal or too shallow, and aggressive flap elevation. The honest defense is prevention through case selection and three-dimensional position, supported by buccal gap grafting and, where indicated, a connective tissue graft. Once recession has established itself around an osseointegrated implant it is one of the hardest problems in implant dentistry to reverse, which is why the threshold for accepting a borderline esthetic case should be high.
Loss of primary stability is a surgical-day problem with a simple answer: if the implant does not seat with stability in the position the restoration needs, do not place it. Convert to socket preservation and a delayed implant rather than forcing an unstable implant to probably integrate.
Malposition is the complication the socket itself tries to create, because the path of least resistance for the drill is straight down the old root, which is usually too buccal and too deep. Start the osteotomy against the palatal wall and use the restorative plan, and where appropriate a surgical guide, to define the axis. Infection, finally, is a contraindication when acute and uncontrolled, and a manageable variable when chronic and debrided: thorough curettage and sound judgement about the residual bacterial load decide whether the case proceeds today or waits.
What The Evidence Should Make Us Humble About
Systematic reviews and consensus statements generally support high survival rates for immediate and early implants in selected cases, but they are equally clear that survival is the easy outcome to hit and esthetics is the hard one. An implant can be fully osseointegrated and counted as a success in a survival table while sitting behind a visibly receded margin the patient considers a failure. That gap between survival and esthetic success is the single most important thing the evidence asks us to be humble about, and it is why recession risk, not loss of the implant, dominates the risk discussion for anterior immediate placement (Chen and Buser, 2009, ITI Consensus: Implants in Postextraction Sites).
The second lesson is that the favorable results in the literature come from favorable cases: studies reporting excellent esthetics selected intact sockets, thick phenotypes, and ideal positions, and often added gap grafting and soft-tissue augmentation. Reading those results as a license to place immediately in every socket inverts the logic. The outcomes are good because the selection was strict, not because the timing is forgiving. This is why I do not teach immediate placement as a shortcut. I teach it as a discipline, where the protocol and the case selection are the reason the numbers hold up. Fast treatment is valuable only if the result ages well.
What This Guide Does Not Solve
This guide does not replace surgical training, CBCT planning, or prosthetic planning. It is a decision framework, not a substitute for hands and judgement at the chair. It also does not argue that immediate placement is better than early or delayed placement. In many esthetic-zone cases, early placement after several weeks of soft-tissue healing is the more controlled choice, because it gives you keratinized tissue, a partially modeled but still favorable ridge, and a clearer read on infection. The timing decision is a spectrum, and immediate placement is one well-defined point on it, not the destination.
The best immediate implant case is the one where you would still be comfortable with the decision five years later, looking at the margin, the papillae, and the radiograph, with the patient smiling. If a socket cannot give you reasonable confidence in that five-year picture, the most advanced thing you can do is wait, rebuild, and place into a site you have made predictable.
Go Deeper
For the bone and gap-management logic behind immediate implants, the deeper reference is the guided bone regeneration protocol, which covers membrane selection, fixation, and the contained-versus-non-contained defect logic that decides how the jumping gap is handled. For the surgical workflows, socket classification, soft-tissue management, and worked video cases in one guided format, the interactive Immediate Implants ebook walks through the decisions in this article step by step.
References
Frequently Asked Questions
What is immediate implant placement?
Immediate implant placement means placing a dental implant into a fresh extraction socket at the same appointment as the tooth extraction. It is also called Type 1 placement. It does not automatically mean immediate loading or immediate provisionalization, which are separate decisions with their own requirements.
When is immediate implant placement appropriate?
It is appropriate when case selection is favorable: infection is controlled, the socket walls allow an ideal three-dimensional implant position, primary stability is achievable in apical and palatal or lingual bone, and soft-tissue and esthetic risk are acceptable. When the buccal wall is missing or too thin, early or delayed placement after augmentation is usually the more controlled choice.
Is immediate implant placement predictable?
It can be predictable in carefully selected cases, but it is technique-sensitive and case-selection sensitive. Survival rates are generally high, while esthetic outcomes are more variable. Poor socket walls, infection, a thin phenotype, malposition, or weak primary stability all increase the risk of recession and a compromised result.
What is the jumping distance?
The jumping distance is the horizontal gap between the implant surface and the inner wall of the fresh extraction socket, most relevant on the buccal aspect. It is the expected result of positioning the implant toward the palatal or lingual wall for stability and correct restorative position, not a placement error.
Should the buccal gap be grafted?
In many immediate implant cases the buccal gap is filled with a slow-resorbing graft to support the ridge contour and compensate for post-extraction modeling. The decision depends on gap size, buccal wall thickness, and defect morphology. A small contained gap behind a thick wall may be monitored, while a dehiscence should be treated as a guided bone regeneration defect rather than a simple gap fill.
Is immediate placement the same as immediate provisionalization?
No. Immediate placement refers only to inserting the implant on the day of extraction. Immediate provisionalization, placing a non-loaded temporary crown the same day, additionally requires genuine primary stability, a controllable occlusion with no contacts on the provisional, and a good implant position. If those are not all present, a healing abutment or a delayed provisional is safer.
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
Guided Bone Regeneration: A Clinical Guide to Every Bone Defect
Next
Peri-implantitis Treatment: Diagnose the Defect Before You Treat the Implant
Related Articles
5 Concepts to Achieve a Successful Immediate Implant Placement Into a Fresh Molar
10 min read
Immediate Implants in the Aesthetic zone: Some tips and tricks that will help you
19 min read