The Connective Tissue Graft: Harvesting Techniques, Indications, and CTG vs FGG

Table of Contents
Related clinical guides
The connective tissue graft is one of those procedures that looks small until you understand what it controls.
A few millimeters of tissue can decide whether a root-coverage case blends or looks patched. It can decide whether an implant crown looks natural or gray. It can decide whether the patient can clean the area comfortably. And it can decide whether the surgeon spends the afternoon relaxed or negotiating with the greater palatine artery.
I like CTG because it is honest surgery. You cannot hide from anatomy. You cannot hide from flap thickness. You cannot hide from tension. The palate gives you what it gives you, and your job is to harvest enough tissue without being greedy.
Connective Tissue Graft Technique And Soft Tissue Grafting Around Implants
In practice, the question is not only "what is a CTG?" The useful decision is when a connective tissue graft technique adds thickness, when soft tissue grafting around implants improves the peri-implant envelope, when palatal harvesting is justified, and when an FGG is the better tool than a CTG.
For coverage of exposed roots, coronally advanced flap with subepithelial connective tissue graft remains one of the key reference approaches in the literature (Chambrone et al., 2022). For implant dentistry, the question shifts from coverage of exposed roots to phenotype: can we increase soft-tissue thickness, improve contour, and make the restoration easier to maintain? A systematic review and network meta-analysis on peri-implant soft-tissue phenotype modification is a useful authority link for that discussion (Tavelli et al., 2021).
That is why I do not teach palatal harvesting as a trick. I teach it as anatomy plus indication plus wound management.
What A CTG Is Actually For
A CTG is autogenous connective tissue, most often harvested from the palate and placed under a flap or into a recipient pouch. The surface epithelium is not the objective. The objective is the connective tissue volume and biology underneath.
I use CTG for four main reasons:
- Coverage support for exposed-root defects in recession defects with a realistic prognosis.
- Soft-tissue thickening around teeth or implants.
- Esthetic blending where a free gingival graft would be too visible.
- Peri-implant phenotype management when thin tissue puts the reconstruction at higher esthetic or maintenance risk.
The evidence around recession treatment still supports the combination of coronally advanced flap and subepithelial connective tissue graft as a strong reference approach for single exposed-root defects Chambrone et al., 2022. Around implants, soft-tissue augmentation procedures can increase tissue thickness, and CTG remains an important benchmark Valles et al., 2022.
CTG vs FGG: Do Not Confuse The Jobs
| Question | CTG | FGG |
|---|---|---|
| Main goal | Thickness, volume, esthetic blending | Keratinized tissue width |
| How it heals | Buried under a flap or pouch | Exposed surface heals by secondary intention |
| Esthetic behavior | Usually blends better | More likely to show color/texture mismatch |
| Donor morbidity | Often primary closure possible | Open palatal wound is more common |
| Best use | Coverage of exposed roots, implant soft-tissue thickening, contour | Increase attached/keratinized mucosa where esthetics are secondary |
A free gingival graft is not an inferior CTG. It is a different tool. If the patient needs keratinized tissue width in a non-esthetic posterior site, FGG may be the more honest option.
The Palate Is The Real Boss
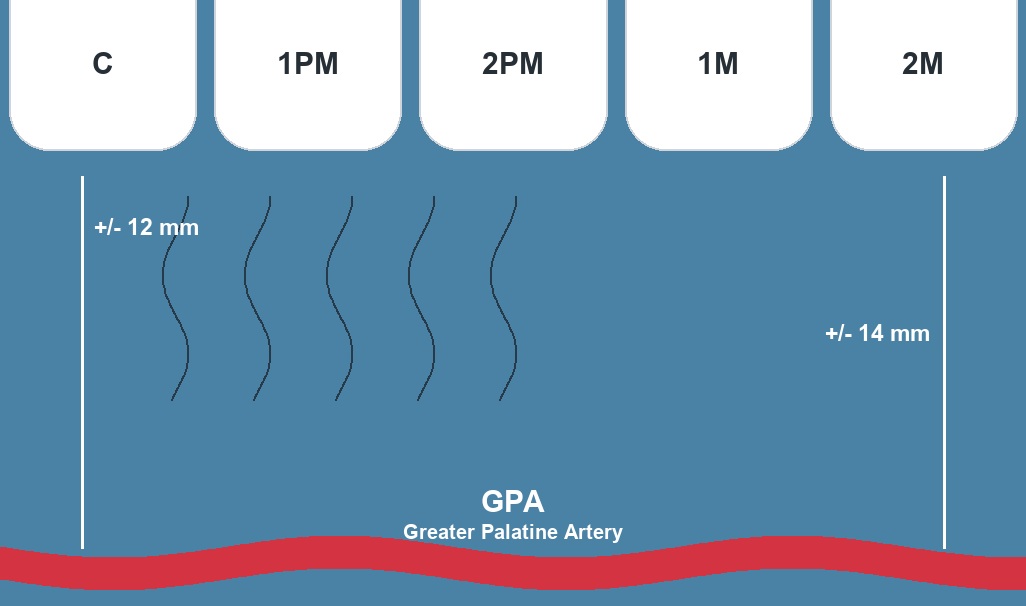
The danger is not theoretical. The greater palatine artery travels anteriorly from the greater palatine foramen, and its position matters when you plan graft height and length. Anatomical studies of the palate are useful because they remind us that graft size is not only a surgical preference Klosek and Rungruang, 2009.
In a practical sense:
- A high, thick palate gives more vertical room.
- A shallow palate brings the neurovascular bundle closer to the harvest zone.
- The first molar region and posterior palate require extra respect.
- A very thin palate is not a place to prove courage.
This is where the problem starts: clinicians often choose a technique first and inspect the donor anatomy second. I prefer the reverse.
Harvesting Techniques And When I Use Them
Surgical video: choose the harvest after you respect the anatomy.
These videos are useful here because harvesting is not an abstract technique choice. The palate, the phenotype, the recipient site, and the closure all decide how aggressive you can be.
Trap-door or double-incision harvest
Here I make a horizontal outer incision parallel to the gingival margin, then a second deeper incision to raise a partial-thickness palatal flap, lift that flap as a "trap door," and remove the connective tissue underneath before laying the flap back down. The advantage is generous tissue volume and good visibility of the plane I am working in, especially when the palate is favorable. The price is more flap management at the donor site and a partial-thickness flap that must stay perfused, so I keep the outer flap of even thickness and avoid buttonholing it. The first incision sets the depth of the outer flap, the second defines the block I take, and the apical extent stays above the artery.
I consider it when I need volume and the vault gives me the vertical space to take a true block without crowding the neurovascular bundle. Closure is by primary intention over the harvested bed, which is one of its real attractions: the surface is replaced rather than left open.
Single-incision harvest
The single-incision technique uses one linear access cut, then a split-thickness undermining of the overlying tissue to dissect the connective tissue out through that single line. It is useful when I want a smaller access wound and primary donor closure, because the access incision is closed directly with simple interrupted or a continuous suture and the palate heals largely by first intention. It can reduce donor-site morbidity and patient discomfort, but it demands precision because you see less: the dissection is essentially blind, so blade angulation and a consistent plane matter more than in the open trap-door approach.
I consider it when the volume need is moderate and I want a cleaner closure. The trade-off is real, and it is worth comparing the access techniques side by side, which I cover in more detail in four connective tissue harvesting techniques.
De-epithelialized free gingival graft
This gives dense, fibre-rich tissue and can be very useful, but the donor-site wound behaves differently. You harvest a free gingival graft as usual, then de-epithelialize it extraorally with a fresh blade on a stable surface until the keratinized surface is gone and only lamina propria remains. The advantage is a thick, uniform graft with predictable connective tissue density. The cost is an open secondary-intention palatal wound rather than a primarily closed access, so I reserve it for cases where I genuinely need that density and the patient can tolerate the donor-site course. It is not automatically more elegant than a buried single-incision harvest. It is simply another way to get the tissue, with a different wound to manage.
How thick should the graft be?
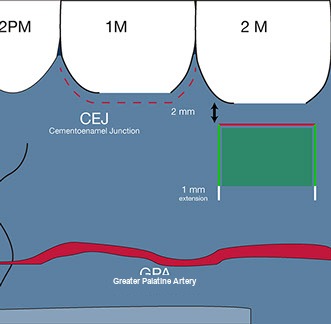
Before the technique, decide the target. For root coverage under a coronally advanced flap or a tunnel, I aim for a graft on the order of 1 to 1.5 mm thick: thick enough to add phenotype and resist relapse, thin enough to revascularize through the overlying flap without compromising the most superficial fibres. For ridge or peri-implant volume, where the graft sits in a deeper envelope, I accept a thicker block because the priority is contour rather than translucent coverage. A graft that is too thin tears during suturing and adds little phenotype. A graft that is too thick outruns its blood supply, sloughs at the surface, and undermines the donor site. The thickness decision is made by reading the palate first, then choosing the technique that can deliver it safely.
Reading the safe harvest window
The working rule on the palate is conservative. I stay a short distance, roughly 2 mm, away from the gingival margin of the donor teeth so the marginal tissue and its blood supply are preserved, and I keep the apical extent of the harvest above the level where the greater palatine artery and its branches run. The artery emerges from the greater palatine foramen near the second and third molars and travels anteriorly in the submucosa of the lateral palate, so the height of safe tissue shrinks as you move posteriorly and as the vault flattens. In a high, vaulted palate there is generous vertical room between the gingival margin and the neurovascular bundle. In a shallow, flat palate that corridor narrows quickly, and the honest move is a smaller graft, a different donor area such as the maxillary tuberosity, or a staged plan rather than a deep cut over the artery.
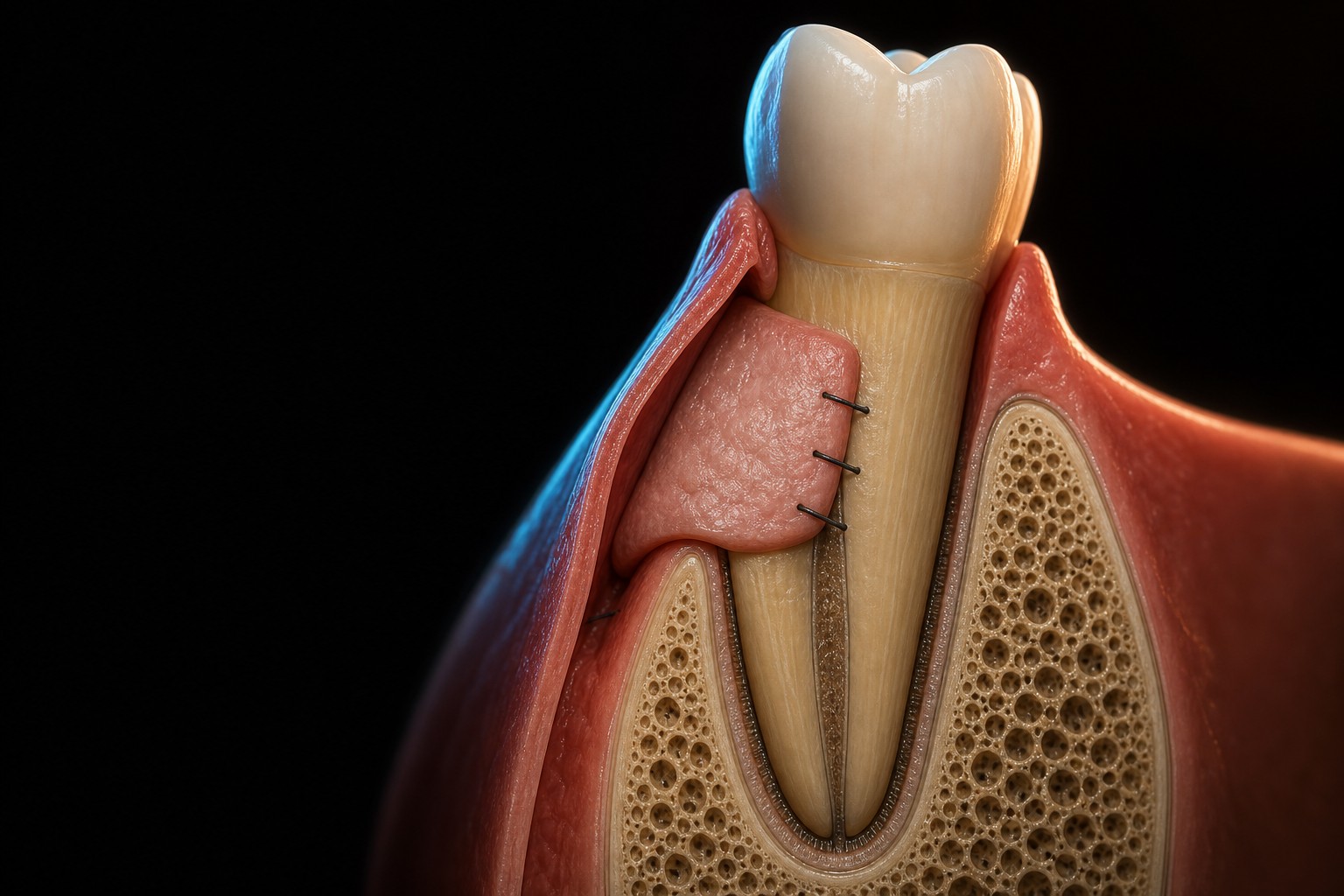
Graft handling and recipient-site suturing
Once the graft is out, handle it as little as possible and keep it moist in saline while you prepare the recipient bed. Orient it so the periosteal or deepest connective-tissue surface faces the bone or root and the cut surface faces the flap, which favors revascularization. Immobility is everything: a graft that moves does not take. I stabilize it with fine resorbable or non-resorbable sutures, sling or anchor sutures to fix it against the recipient bed, and then advance the overlying flap to cover as much of the graft as the case allows. Passive tension is the goal, because a flap closed under tension pulls the margin back and starves the graft at its most superficial layer. Coronal advancement, periosteal release where needed, and tension-free closure decide whether the thickness you harvested actually stays where you put it.
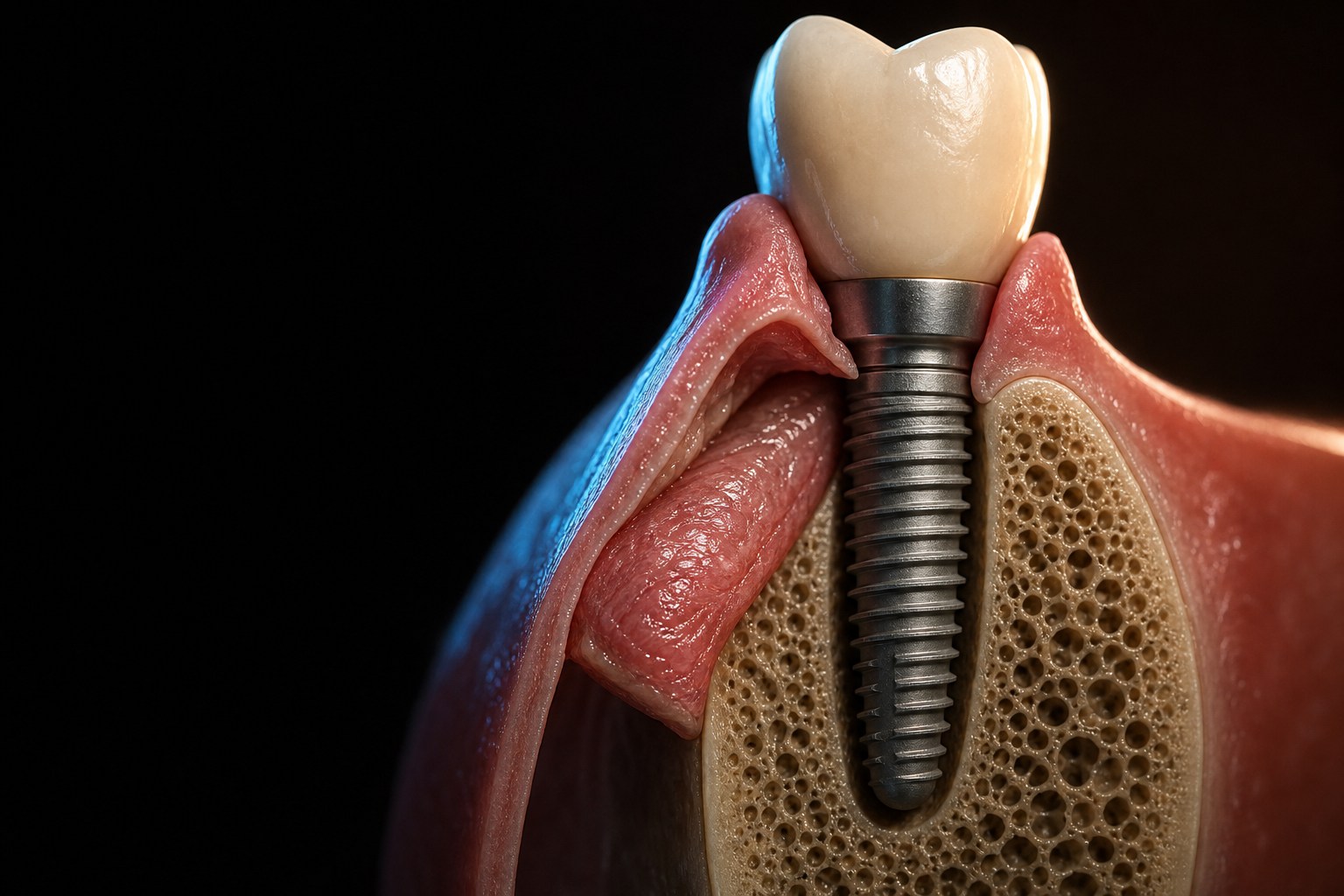
Around Implants, CTG Is Not Decoration
Thin peri-implant tissue can make the gray shine through, expose restorative margins, increase recession risk, and make hygiene less comfortable. CTG can help thicken the envelope, especially in the esthetic zone or around immediate implant placement, where the soft-tissue envelope has to hold its shape during early healing. A thicker, more keratinized peri-implant phenotype is also easier to keep healthy and easier to clean, which matters for long-term peri-implantitis prevention and management.
But here is the caveat: CTG does not fix a facially placed implant. It does not replace missing buccal bone. It does not make a bulky restoration cleansable.
Soft tissue and hard tissue are one plan, not two.
Important distinction: when the main problem is deficient buccal hard-tissue contour or lip support, I treat it as a guided bone regeneration and prosthetic-contour diagnosis first. CTG can improve phenotype thickness, but it is not a substitute for rebuilding missing hard-tissue volume.
Donor-Site Management And Complications

The recipient site gets most of the attention, but the donor site is where avoidable problems live. Two things decide donor-site comfort: how cleanly you close it and how well you control bleeding.
For hemostasis, the first move is local pressure with gauze and time, not panic. A palatal stent or vacuum-formed plate worn over the wound stabilizes the clot, protects the area from the tongue and food, and is the single most useful aid for patient comfort in an open palatal wound. Where the technique allows primary closure, sutures over the harvested bed reduce the raw surface and shorten healing. When the wound stays open, as with a free gingival or de-epithelialized harvest, I accept secondary-intention healing and manage it with the stent, a hemostatic dressing if needed, and clear post-operative instructions.
The complication everyone fears is injury to the greater palatine artery. The defense is preventive, not reactive: stay within the safe window, keep the apical extent of the harvest above the artery's course, and treat a flat, shallow palate as the higher-risk anatomy it is. If brisk bleeding does occur, sustained direct pressure controls most events; persistent arterial bleeding needs the wound opened, the vessel identified, and definitive control rather than repeated blind packing.
Other donor-site issues are usually about depth and handling. A flap raised too thin can necrose or buttonhole, so I keep the outer flap even and well perfused. Taking a graft that is too large or too deep slows healing and increases the chance of exposed bone and delayed epithelialization. Post-operative pain, transient sensory disturbance near the harvest, and minor sloughing of an over-thick graft are the common, mostly self-limiting problems, and most of them trace back to one of three decisions made before the first cut: graft size, harvest depth, and respect for the artery.
When I plan donor morbidity, I plan it together with the bone side of the case. The same principle that governs guided bone regeneration applies to soft tissue: protect the blood supply, keep the wound closed where you can, and do not ask a graft to survive in a bed that cannot feed it.
Case Selection And Recession Classification
Case selection is where CTG cases are won or lost, and recession classification is the language for it. The older Miller classification and the newer Cairo system (recession types RT1, RT2, RT3) both turn on the same clinical question: how much interproximal attachment and papilla height remain. When the interdental tissue is intact, as in a Cairo RT1 or a favorable Miller class, complete root coverage is a realistic goal and a CTG under a coronally advanced flap or tunnel is doing what it does best. When interproximal attachment is already lost, as in RT2 or RT3, full coverage becomes unpredictable, and I tell the patient that before I tell them anything else.
The phenotype decides how the graft behaves. A thick, well-keratinized phenotype is forgiving and may not even need a graft for a shallow defect. A thin phenotype is exactly where the added thickness earns its keep, both for immediate coverage and for long-term stability of the margin. Plaque control, smoking, and the patient's esthetic demands belong in this conversation too, because a technically perfect graft on an uncontrolled mouth is a short-term result. The graft respects biology; it does not override it.
My Practical Selection Framework
| Situation | More likely graft choice | Reason |
|---|---|---|
| Esthetic coverage of exposed roots with thin phenotype | CTG under CAF or tunnel | Thickness and blending |
| Posterior site lacking keratinized mucosa | FGG | Width matters more than color match |
| Immediate implant in thin biotype | CTG with careful bone/gap management | Supports the soft-tissue envelope |
| Ridge contour deficiency | CTG or substitute depending on volume and patient factors | Volume augmentation |
| Shallow palate with limited tissue | Smaller CTG, alternative donor site, or staged plan | Safety first |
What This Guide Does Not Solve
A CTG is not a universal patch. It will not make a recession defect with severe interproximal attachment loss behave like a simple Miller/Cairo favorable recession. It will not make poor plaque control disappear. It will not fix implant malposition.
The graft is powerful because it respects biology. It fails when we ask it to hide bad planning.
Go Deeper
For the bone-side of this problem, study the interactive Guided Bone Regeneration ebook. For immediate implant soft-tissue sequencing, use the Periospot immediate implant material and CTG case videos in the library.
The most useful habit is simple: decide the bone envelope and the soft-tissue envelope together before the first incision.
References
- Chambrone L, Botelho J, Machado V, Mascarenhas P, Mendes JJ, Avila-Ortiz G. Does the subepithelial connective tissue graft in conjunction with a coronally advanced flap remain as the gold standard therapy for the treatment of single gingival recession defects? A systematic review and network meta-analysis. J Periodontol. 2022 Sep. PMID 35451068
- Valles C, Vilarrasa J, Barallat L, Pascual A, Nart J. Efficacy of soft tissue augmentation procedures on tissue thickening around dental implants: A systematic review and meta-analysis. Clin Oral Implants Res. 2022 Jun. PMID 35763023
- Tavelli L, Barootchi S, Avila-Ortiz G, Urban IA, Giannobile WV, Wang HL. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: A systematic review and network meta-analysis. J Periodontol. 2021 Jan. PMID 32710810
- Klosek SK, Rungruang T. Anatomical study of the greater palatine artery and related structures of the palatal vault: considerations for palate as the subepithelial connective tissue graft donor site. Surg Radiol Anat. 2009 Apr. PMID 19015806
Frequently Asked Questions
What is a connective tissue graft?
A connective tissue graft is an autogenous soft-tissue graft, usually harvested from the palate, used to increase tissue thickness, improve root coverage, or strengthen peri-implant soft tissue.
What is the difference between CTG and FGG?
A CTG is buried under a flap and is mainly used for volume, thickness, and esthetic blending. A free gingival graft remains exposed and is mainly used to increase keratinized tissue width.
Where is a CTG harvested from?
Most connective tissue grafts are harvested from the palate, but the safe harvest dimensions depend on palatal vault shape, tissue thickness, and the course of the greater palatine artery.
Is CTG useful around implants?
Yes, CTG can increase soft-tissue thickness around implants and support esthetic and maintenance goals, but it does not compensate for poor implant position or missing bone.
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
Dental Video Marketing in 2026: How to Make Pro Videos Without a Video Editor
Next
Guided Bone Regeneration: A Clinical Guide to Every Bone Defect