Peri-implantitis Treatment: Diagnose the Defect Before You Treat the Implant


Table of Contents
Related clinical guides
If you place implants, then sooner or later you'll be staring at a bleeding, deepening pocket around one of them, and the honest first step in peri-implantitis treatment is not reaching for a laser or a bone graft. It's picking up a probe and asking one question: what am I actually treating? I've watched too many colleagues (and earlier versions of myself) jump straight to a technique before they've defined the disease. That's backwards. The technique is the last decision, not the first.
So let's slow down and build this from diagnosis up.
Short answer: Peri-implantitis treatment is a sequence, not a single procedure. You confirm the diagnosis with probing and radiographs, control the cause non-surgically, re-evaluate against clear endpoints, and only then decide whether to do surgery, which kind, and whether the implant is even worth saving. The technique you pick matters far less than the order in which you make these decisions.
What peri-implantitis is, and what it is not
The 2017 World Workshop gave us shared language here, and it's worth using precisely because sloppy terminology leads to sloppy treatment.
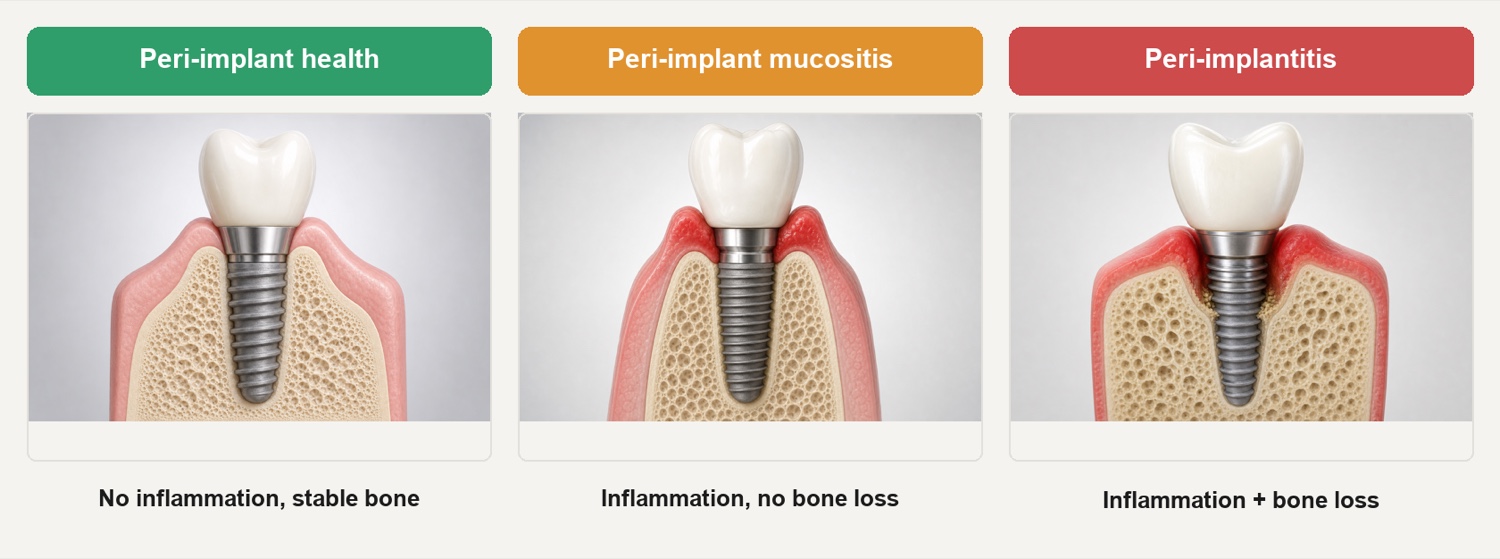
Peri-implant mucositis is plaque- or biofilm-induced inflammation of the soft tissue around an implant, with bleeding on probing, but without progressive bone loss beyond initial remodeling. It's the gingivitis analog, and the critical word is reversible. Remove the biofilm, fix the access, and the tissue can return to health.
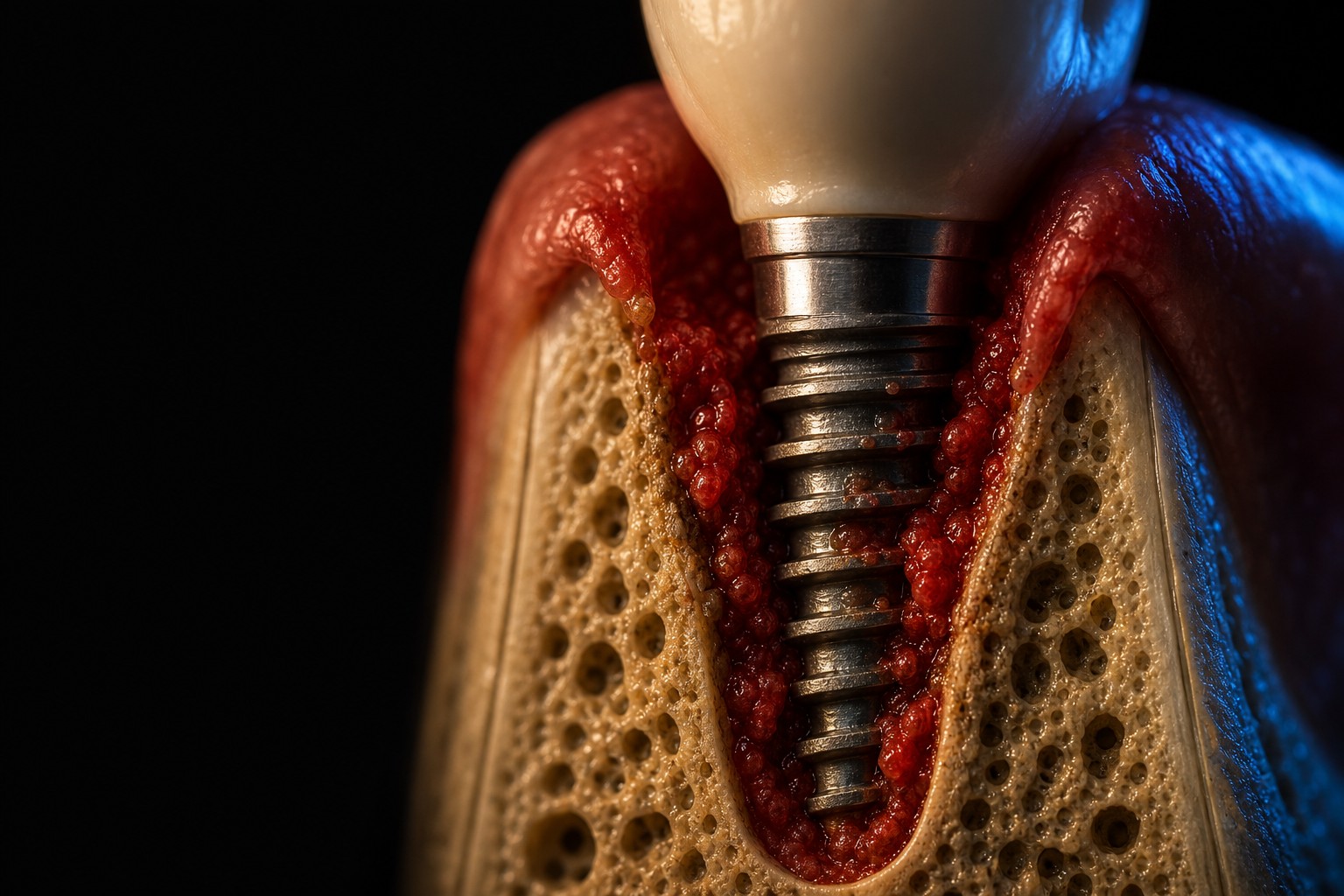
Peri-implantitis is mucositis plus progressive bone loss. It's the periodontitis analog, except worse in one important way: untreated peri-implantitis progresses non-linearly and faster than periodontitis (Berglundh 2018; Schwarz 2018). You don't get the slow, semi-predictable decline you might expect from a periodontal pocket. You get quiet stretches followed by sudden drops. That's why early, confident diagnosis matters so much.
The case definitions, with actual numbers
This is where most chairside confusion lives, so let me be exact. The Renvert et al. 2018 case definitions (J Clin Periodontol) split on one question: do you have baseline records?
If you have baseline data (a radiograph and probing depths from the time of prosthesis delivery), peri-implantitis is:
- Bleeding and/or suppuration on gentle probing, plus
- Increased probing depth compared to the baseline value, plus
- Bone loss beyond the initial crestal remodeling.
If you do not have baseline data (the far more common real-world situation, especially for implants you didn't place), peri-implantitis is defined by absolute thresholds:
- Radiographic bone level at least 3 mm apical to the most coronal portion of the intraosseous part of the implant, plus
- Bleeding on probing, plus
- Probing depth of 6 mm or more.
That 3 mm / 6 mm threshold is a fallback for when history is missing. It is not a universal definition. If you have baseline films, use them, because change over time is more meaningful than any single absolute number.
How common is this, really
Prevalence numbers for peri-implantitis are all over the map, and I'd rather you understand why than memorize one figure that sounds authoritative.
The range exists because studies have used different case definitions, different bone-loss thresholds, and different populations. When the goalposts move, the prevalence moves with them. Here's the spread from the major reviews:
| Source | Mucositis | Peri-implantitis |
|---|---|---|
| Derks & Tomasi 2015 | ~43% (patient-level) | ~22% (patient-level) |
| Lee 2017 | not reported here | ~19.8% subject / ~9.3% implant |
| Diaz 2022 | not reported here | ~19.5% patient / ~12.5% implant |
Read those as a band, not a point. Roughly one in five patients with implants, and somewhere around one in ten implants, is a reasonable mental model. Patient-level numbers always run higher than implant-level numbers, because a patient with one affected implant counts as a case even if their other implants are healthy. When someone quotes you a single confident percentage for peri-implantitis prevalence, ask which case definition they used. The answer usually explains the number.
Risk indicators, not proven causes
I'm deliberate about this word. Most of what we know about who gets peri-implantitis comes from observational data, which can show association but not prove causation. So these are risk indicators, things that travel with the disease, not certified causal factors. Treat them as flags that raise your index of suspicion and shape your maintenance planning, not as switches that flip the disease on.
The two strongest and most consistent indicators are a history of periodontitis and smoking. Even those remain observational.
| Risk indicator | Reported odds ratio | Notes |
|---|---|---|
| History of periodontitis | ~2.9 (4.0 if active disease) | Strongest, most consistent indicator |
| Smoking | ~2.3 | Strong, consistent, dose-related in practice |
| Poor plaque control / no maintenance | strong (single-study estimates only) | The biggest modifiable signal |
| Lack of keratinized mucosa (<2 mm) | ~2.78 | Mahardawi et al., 2023 |
| Residual or excess cement | local, observational | Local irritant; design out cement margins |
| Diabetes / hyperglycemia | ~2.3 | Glycemic control matters |
(Odds ratios shown are pooled estimates from the AO/AAP systematic review and meta-analysis (Galarraga-Vinueza et al., 2025), with the keratinized-mucosa figure from a dedicated systematic review (Mahardawi et al., 2023). Individual studies report higher and lower values, so treat these as directional rather than deterministic.)
The practical takeaway: the largest signal in that table is the modifiable one. Poor plaque control and erratic maintenance are the strongest modifiable risk indicators we have, and individual studies have reported strikingly high odds ratios for them, though there is no robust pooled estimate. You cannot change a patient's periodontal history, but you can change whether they get cleaned on a sensible interval and whether their prosthesis lets them clean at home.
My diagnostic sequence
Before any treatment decision, I run the same sequence every time. It takes minutes and it prevents the expensive mistake of treating the wrong thing.
- Get a baseline radiograph, or find the old one. Without a film at prosthesis delivery, you're working from the absolute thresholds above. With one, you can measure real change. Always look for the old film first.
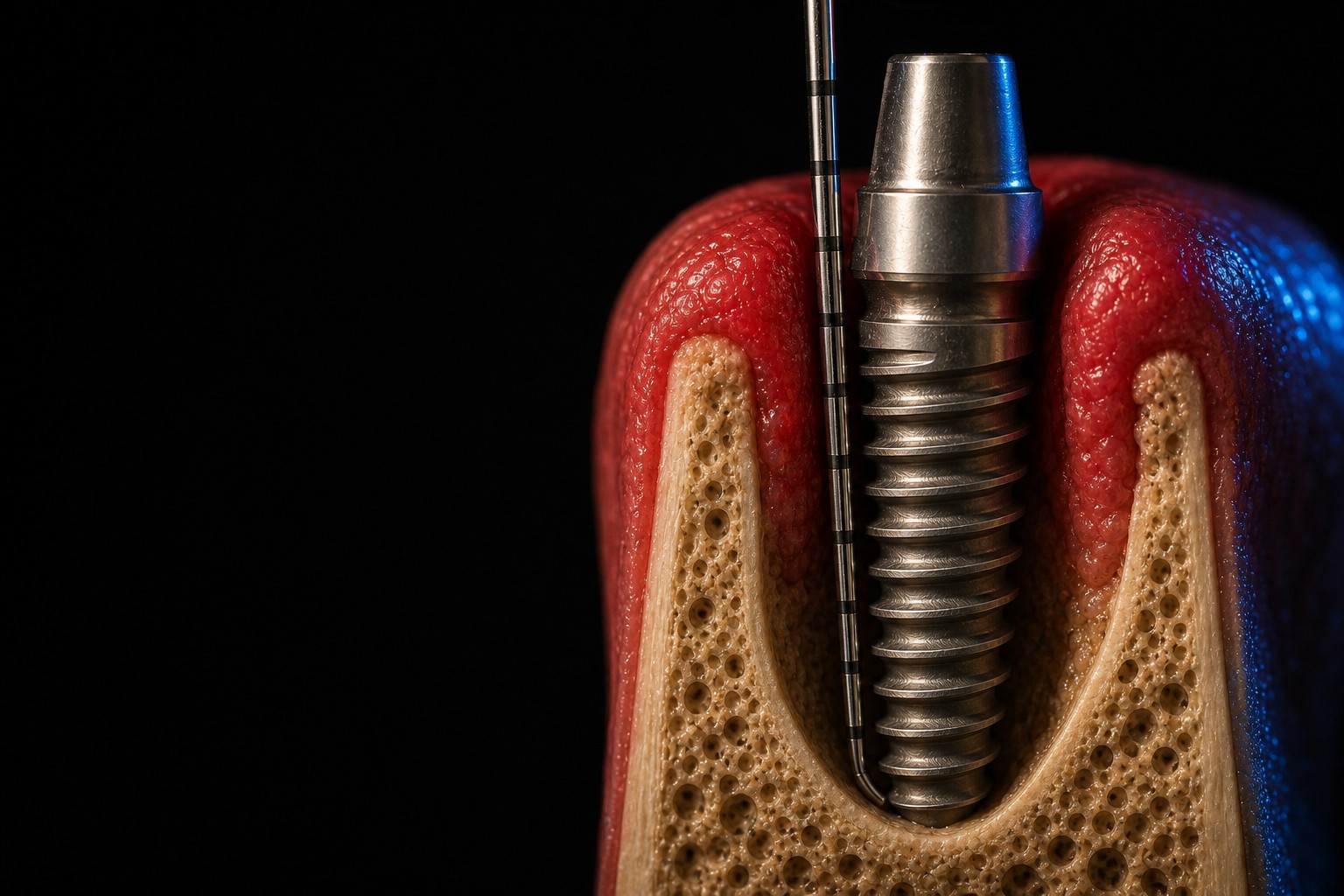
- Probe gently, all the way around. Light force. You're checking for bleeding, suppuration, and depth at six sites. Bleeding on probing is your inflammation signal; depth plus bleeding plus radiographic loss is your disease signal.
- Assess cleansability. Can the patient actually reach this? Can you? An over-contoured crown, a subgingival margin, or a screw-retained bridge with no embrasure access will defeat every technique you try next. Cleansability is often the real diagnosis.
- Read defect morphology. A periapical film tells you there's loss. A CBCT, when justified, tells you the shape of the loss, and shape drives the surgical decision more than depth does.
- Check 3D implant position. A malpositioned implant that can never be cleaned or restored properly changes the entire conversation, sometimes toward explantation.
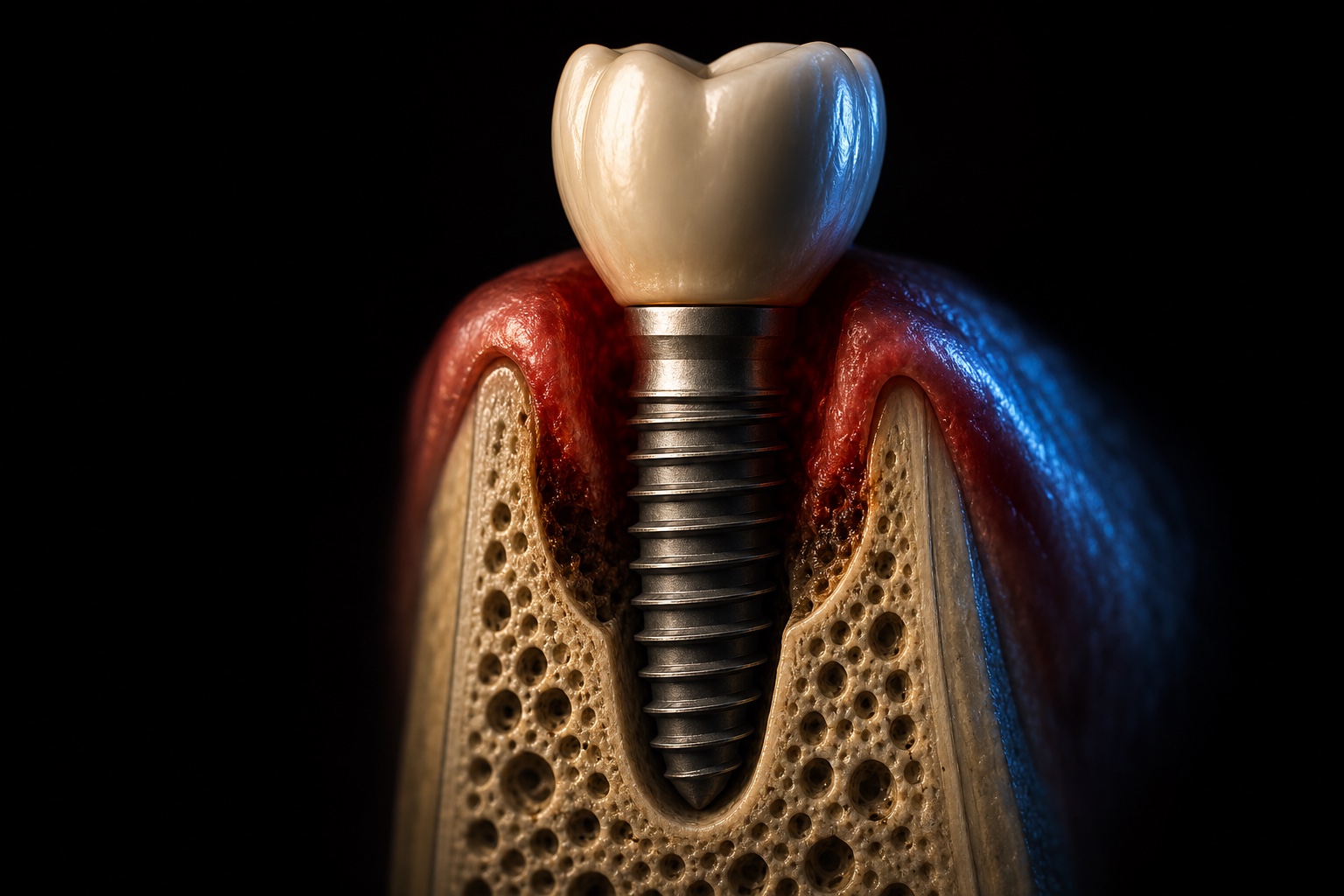
Why defect morphology decides so much
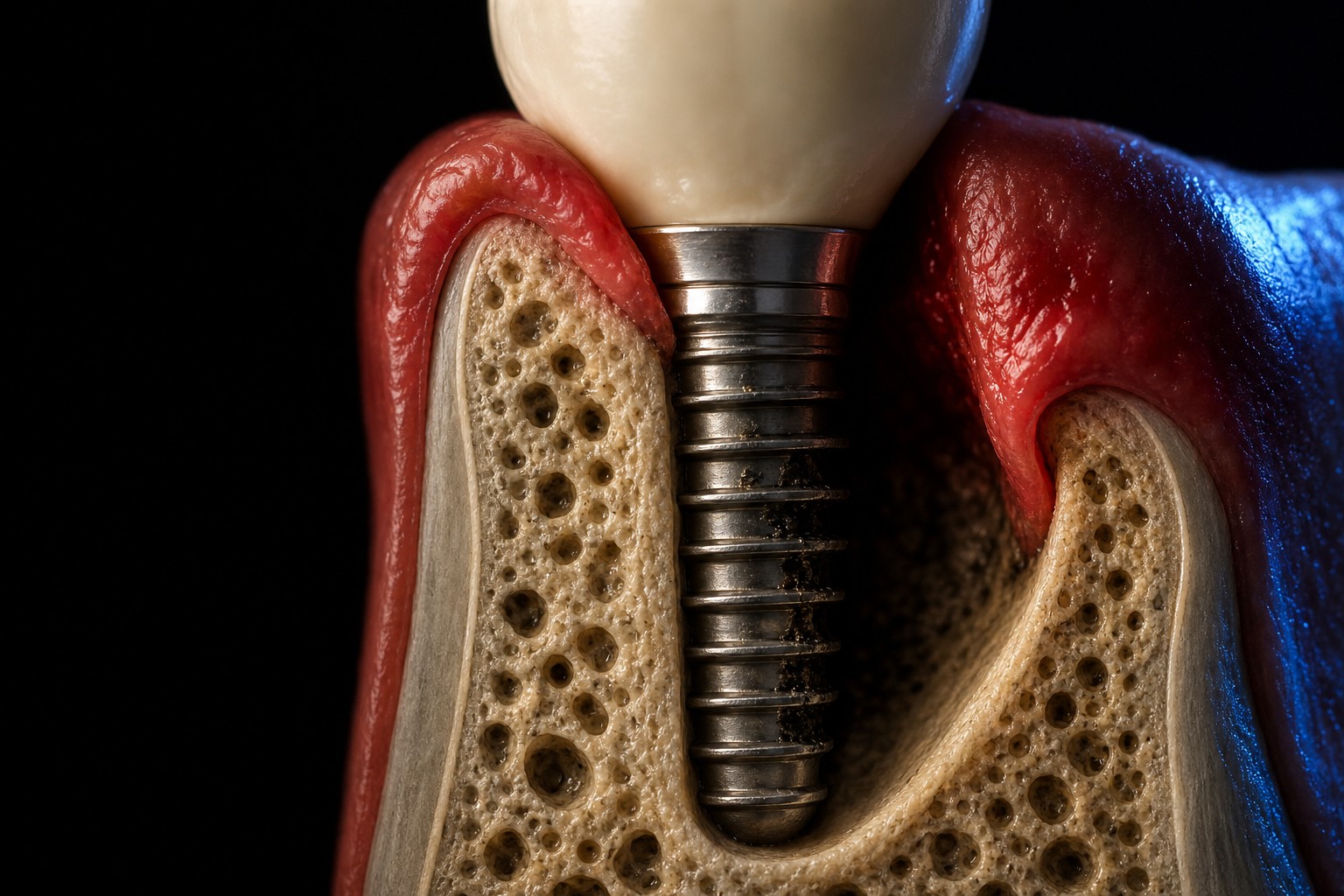
The shape of the bone loss is not a detail, it's a fork in the road. The Schwarz 2007 classification is useful here: a buccal dehiscence alone is a Class Ia defect, while the most common pattern is the circumferential intrabony defect (Class Ie), which accounted for roughly 55% of defects in that series. The key clinical distinction is contained versus non-contained:
- Contained, intra-bony defects hold a graft in place. Bony walls give a regenerative attempt something to work against, and they protect the graft mechanically, the same wall-and-space logic that governs guided bone regeneration around teeth and ridges.
- Horizontal, non-contained loss has nothing to contain a graft. Trying to regenerate here is fighting physics. This is resective or maintenance territory, not reconstructive territory.
Treatment is a sequence: the EFP S3 protocol
Here's the spine of the whole article. The EFP S3 clinical practice guideline (Herrera et al. 2023) lays out a stepwise protocol, and I treat it as the backbone of my decision-making. The point of a stepwise approach is that you don't skip ahead. Each step either resolves the problem or earns you the right to escalate.
Step 0: prevention and getting the basics right
Before anyone has disease, and at every step after, the foundation is the same:
- Design a cleansable prosthesis. If the patient can't clean it, nothing downstream works.
- Ensure adequate keratinized mucosa where it matters.
- Achieve periodontal health before placement. Don't put implants into an uncontrolled periodontal mouth.
- Enroll patients in structured supportive peri-implant care from day one.
Treating mucositis (catch it here if you can)
Mucositis is your best chance, because it's reversible. The guideline is refreshingly simple:
- Professional mechanical biofilm removal, plus
- Reinforced oral hygiene, plus
- Removing prosthetic factors that block access (re-contour or replace the restoration if it's the problem).
What is not recommended for mucositis: adjunctive antibiotics, chlorhexidine, and lasers. They don't earn their place here. Clean it, fix the access, and reinforce home care.
Step 1: non-surgical cause-related therapy for peri-implantitis
When there's bone loss, you still start non-surgically. This step is submarginal instrumentation, oral hygiene reinforcement, and risk-factor control (smoking, glycemic control, the modifiable indicators from the table above). Then you re-evaluate.
Two things the guideline explicitly does not suggest as adjuncts here: lasers, photodynamic therapy, and air-polishing are not suggested, and adjunctive systemic or local antibiotics are not recommended. I know the marketing around these is loud. The evidence is not.
I also think of Step 1 as a stress test. How a patient responds to cause-related therapy tells you whether they'll maintain a surgical result. If they can't or won't engage with non-surgical care and home hygiene, surgery is building on sand.
The re-evaluation endpoint that tells you whether to operate
This is the decision point most people skip. After non-surgical therapy, re-evaluate against a concrete endpoint:
If you achieve a probing depth of 5 mm or less, no suppuration, and bleeding on probing at no more than one site, you do not need to proceed to surgery. Maintain and monitor.
If you don't hit that endpoint, you've earned the surgical conversation. Notice that the decision is driven by a measured outcome, not by how the case looked on day one.
Step 2: surgical therapy, matched to the defect
When the endpoints aren't met, surgery is on the table, and the type of surgery follows the morphology you read earlier:
| If the defect is... | The surgical direction is... | Why |
|---|---|---|
| Horizontal / non-contained | Access flap, resective | Nothing to contain a graft; goal is access and a cleansable architecture |
| Intra-osseous, contained, 3 mm or deeper | Reconstructive (graft +/- barrier membrane) | Bony walls hold and protect the graft |
| Mixed or shallow | Access flap, judgment call | Decontaminate, reduce depth, decide case by case |
A few guideline specifics worth holding onto:
- Access flap is the common denominator. You open to see and to decontaminate.
- Resective approaches fit horizontal, non-contained loss.
- Reconstructive approaches (graft with or without a barrier membrane) are suggested preferably for intra-osseous defects 3 mm or more deep. That depth and containment threshold is the difference between regeneration that has a chance and regeneration that's wishful.
- Implantoplasty (mechanically smoothing the exposed implant surface) has insufficient evidence to recommend for or against. I'm not saying never. I'm saying don't sell it as evidence-based, because it isn't yet.
- Routine systemic antibiotics during surgery are not recommended.
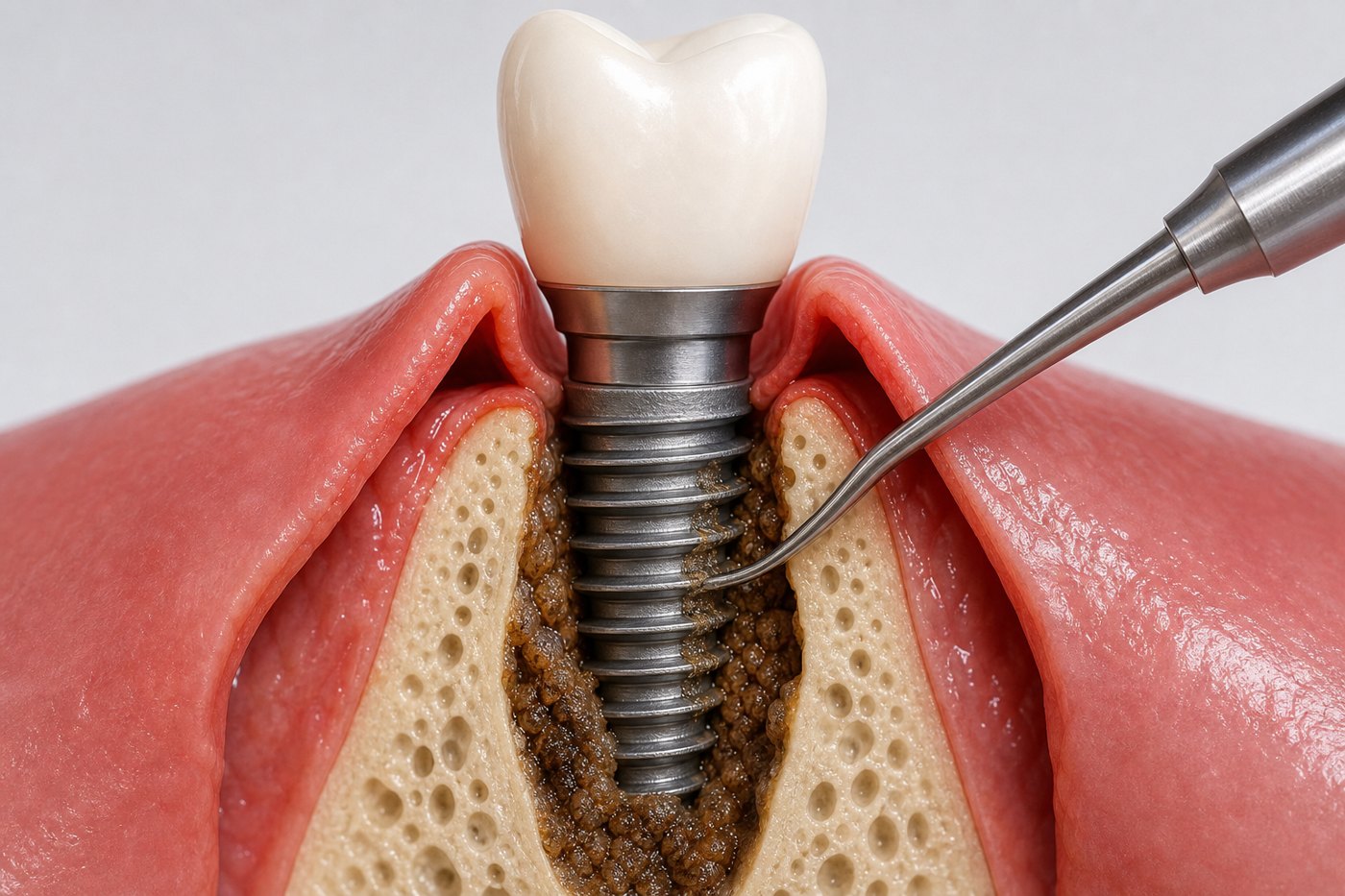
The decontamination toolbox: an honest look
Open ten peri-implantitis surgeries and you'll find ten favorite decontamination protocols, each defended with conviction. Here's the uncomfortable truth from the systematic reviews: no single surface-decontamination method is proven superior to the others, and adjunctive chemical decontamination shows no decisive evidence of better outcomes (Wilensky 2023, a clinical systematic review, with in-vitro/mechanistic support from Hart 2024).
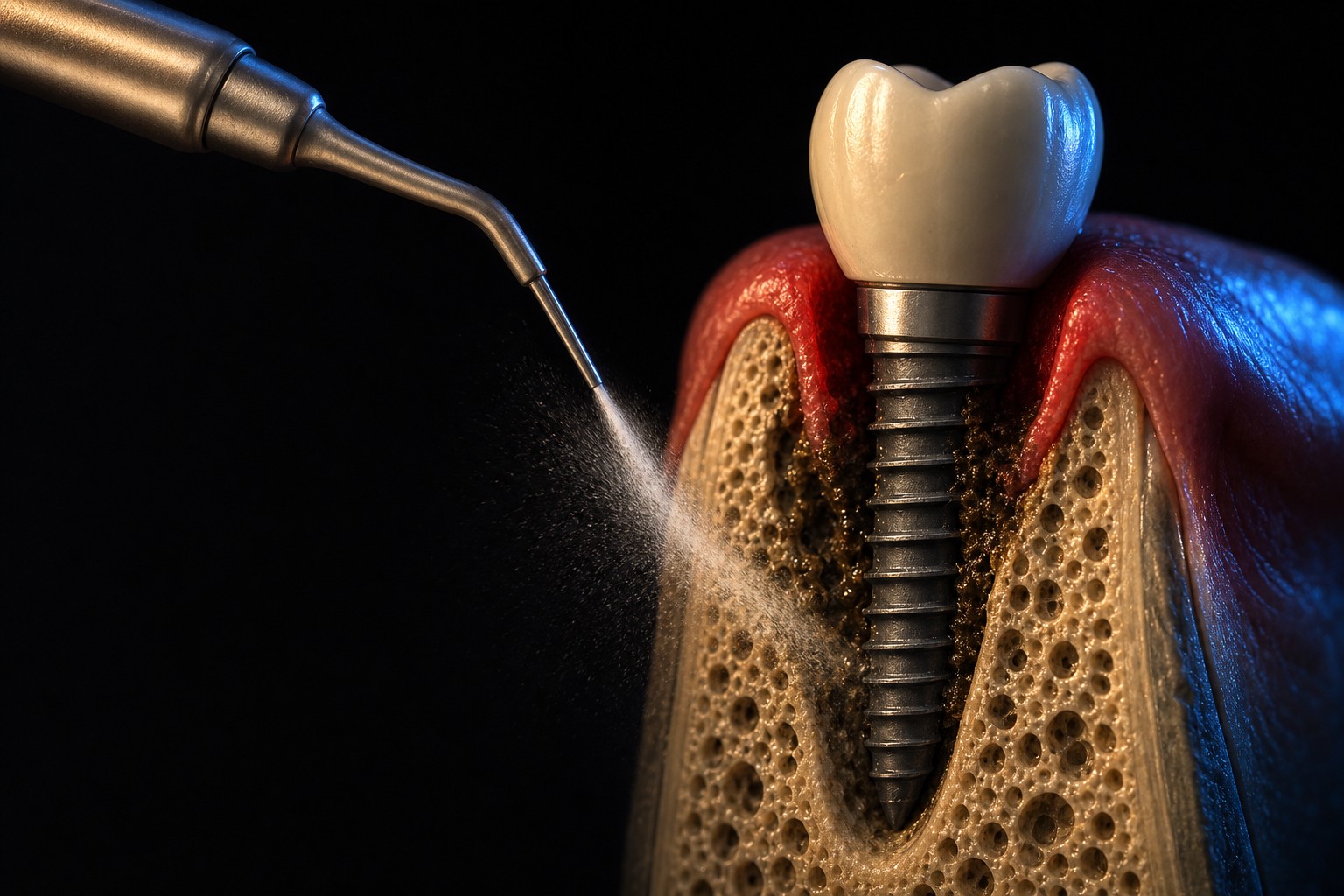
That doesn't mean decontamination is pointless. It means the method is not where the magic is, and you should be skeptical of anyone selling a specific device or chemical as the answer. The EFP position is measured: titanium brushes may be considered, while air-polishing and Er:YAG laser during surgery are not suggested.
My practical stance: use a reasonable mechanical method to clean the surface thoroughly, don't overpay (in money or chair time) for a proprietary protocol that the evidence doesn't elevate above the alternatives, and put your energy into access, defect selection, and maintenance, where the leverage actually is.
Adjuncts: antibiotics and probiotics are not routine
Short section, because the message is short. Systemic and local antibiotics are not recommended as routine adjuncts, for mucositis or for peri-implantitis, surgical or non-surgical. Probiotics, chlorhexidine, and photodynamic therapy don't have the evidence to be standard care either. Reserve antibiotics for specific clinical indications and systemic considerations, not as a reflex add-on to every case. Every unnecessary antibiotic is a cost and a stewardship problem without a matching benefit here.
Regeneration has indications, not guarantees
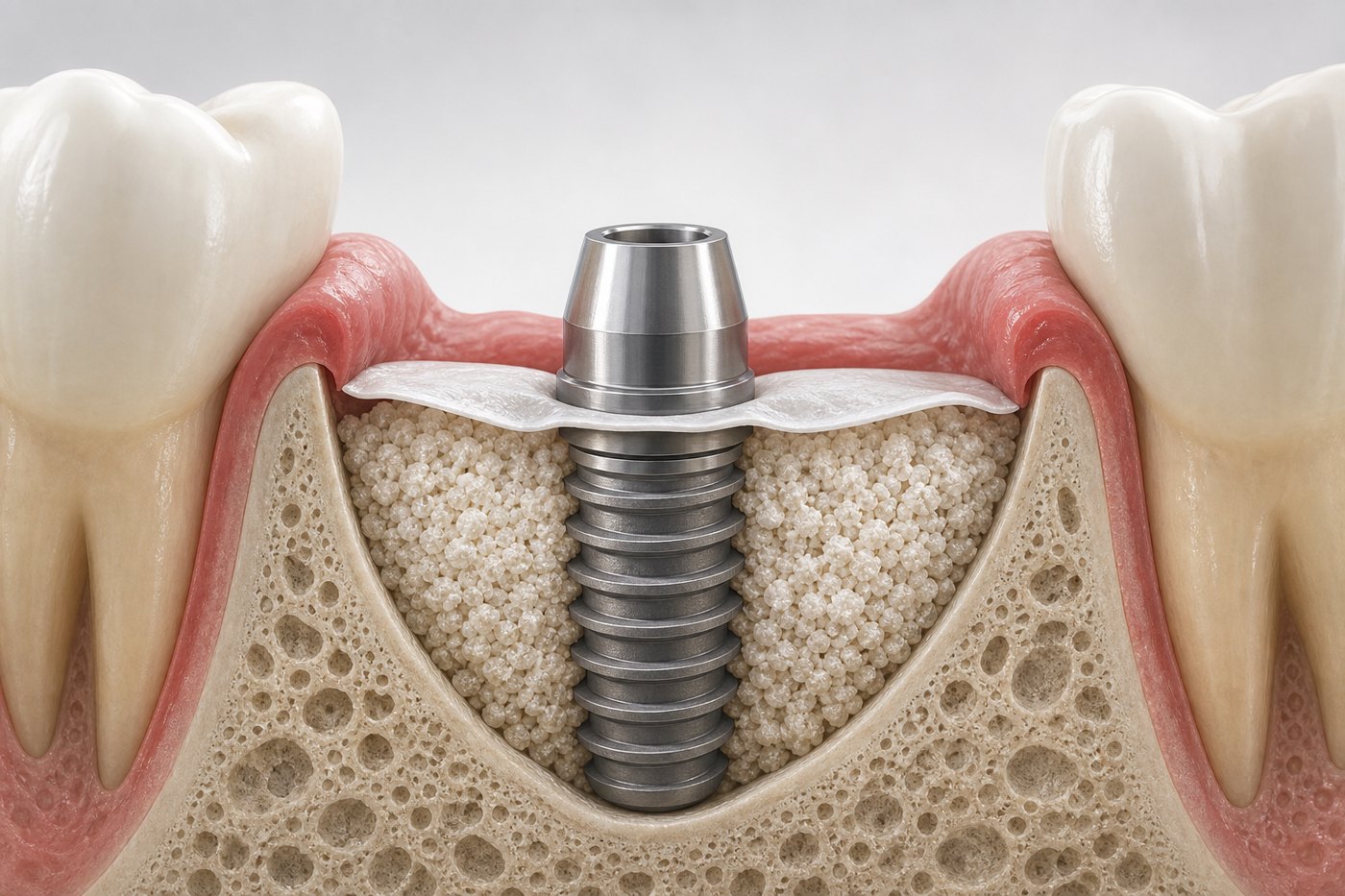
I love a good reconstructive result, but I've learned to manage expectations, my own and the patient's. Regeneration is suggested preferably for contained intra-osseous defects 3 mm or deeper, because those defects hold and protect a graft. Horizontal loss does not qualify.
The honest framing patients deserve: regeneration rarely means true re-osseointegration. You may get radiographic fill and improved probing depths, but bone re-bonding to a previously contaminated implant surface is not something you can promise. When I discuss reconstructive surgery, I describe it as an attempt to improve a defect and the surrounding architecture, not as growing the implant a new foundation.
Realistic outcomes and prognosis
If you take one thing from this article into your consent conversations, take this. Surgical peri-implantitis therapy works, but variably, and recurrence is common.
The numbers (Monje et al., Periodontology 2000, 2025):
- Surgical disease resolution averages around 58.6%, with a wide range from 30% to 98% across studies. That spread is real, not noise: it reflects different defects, patients, and definitions.
- Reconstructive approaches modestly outperform non-reconstructive ones in suitable contained defects. Reconstruction helps in the right defect, but it's not a different universe of success.
- Implant survival after surgical therapy is around 88.6%. Most treated implants are still in the mouth, which is encouraging, but survival is not the same as health.
- Recurrence is common. Two predictors stand out: a residual probing depth of 6 mm or more and keratinized mucosa under 2 mm. Residual pockets raise recurrence odds roughly 8-fold.
Read those together and the strategy writes itself: aim to eliminate residual deep pockets, address keratinized mucosa where it's deficient, and never treat the surgery as the finish line. The residual-pocket finding is the most actionable: if you leave 6 mm pockets behind, the disease is likely to come back.
Go deeper with structured CE. If you want the decision framework behind this article (defect reading, the EFP S3 sequence, and regeneration thresholds) as a guided, interactive learning module, work through the Periospot interactive ebook library. It turns these protocols into step-by-step clinical reasoning you can revisit between cases.
When to stop treating and explant
Not every implant should be rescued, and recognizing that early is a kindness to the patient, not a failure on your part. I move toward explantation when I see:
- Implant mobility. A mobile implant has lost osseointegration; there's nothing to save.
- Advanced bone loss, for example more than 50% of support lost.
- Uncontained defect morphology with poor surface access. If you can't reach and clean the surface, you can't control the disease.
- Malposition that precludes cleansability. A position that can never be maintained is a permanent disease engine.
- Recurrent disease after adequate therapy. If you've done a proper sequence and it keeps coming back, the implant is telling you something.
- Implant fracture.
Chasing a doomed implant through repeated surgeries costs the patient bone, money, and trust. Sometimes the best peri-implantitis treatment is a clean explant and a fresh plan.
Maintenance is part of the treatment, not an afterthought
Everything above collapses without supportive peri-implant care. Poor maintenance is the strongest modifiable risk indicator in the whole picture, and structured recall is the cheapest, highest-leverage thing you can do.
The interval: minimum every 5 to 6 months, risk-adjusted. Longer recall intervals are associated with higher peri-implantitis incidence (Monje 2016). Higher-risk patients (periodontitis history, smokers, poor controllers) come in more often, not less. Maintenance isn't a service you offer at the end; it's structurally part of the treatment, and it starts the day the prosthesis goes in.
A short prevention checklist
If you'd rather prevent this than treat it (you would), this is the day-one checklist:
- Achieve periodontal health before placement. Don't implant into active disease.
- Place implants in a 3D position that can be cleaned and restored, not just one that hits bone. The same prosthetically driven discipline matters most in immediate implant placement, where position is locked in at the time of extraction.
- Ensure adequate keratinized mucosa (the <2 mm threshold carries an OR around 2.78); where it's deficient, a connective tissue graft can rebuild a band of stable, cleansable tissue.
- Deliver a cleansable prosthesis with accessible embrasures and no cement traps.
- Eliminate residual or excess cement. It's a local, avoidable irritant.
- Address modifiable risk indicators: smoking cessation support, glycemic control.
- Enroll every patient in structured supportive care from day one, risk-adjusted to a 5 to 6 month minimum.
Honest truth
Peri-implantitis treatment is less about owning the right device and more about making the right decisions in the right order. We don't have a decontamination method that's proven best. We don't have evidence that implantoplasty works. We can't promise re-osseointegration. Surgical resolution sits around 58.6% with a huge range, and recurrence is common, especially when you leave deep pockets behind. Some implants shouldn't be rescued at all, and recognizing those early is part of doing this well, not a defeat.
What we do have is a clear sequence: diagnose precisely, control the cause, re-evaluate against a clear endpoint (probing depth of 5 mm or less, no suppuration, and bleeding at no more than one site), match surgery to the defect, and maintain relentlessly. That sequence, done honestly, beats any single technique applied confidently to the wrong case. If you remember nothing else: define the disease before you pick the tool, and tell the patient the truth about what surgery can and can't do.
FAQ
What is peri-implantitis?
Peri-implantitis is inflammation around an implant associated with progressive supporting bone loss after initial healing.
Can peri-implantitis be treated without surgery?
Early or less advanced inflammatory cases may start with non-surgical cause-related therapy, but established peri-implantitis often needs surgical access when closed debridement cannot control the defect.
When is regeneration considered in peri-implantitis?
Regeneration is considered mainly in selected contained intrabony defects after decontamination and cause control, when the defect can protect the graft and membrane.
When should an implant be removed?
Implant removal should be considered when the implant is malpositioned, uncleanable, structurally compromised, or surrounded by a defect that cannot be maintained predictably.
Key references
- Galarraga-Vinueza et al. 2025, Prevalence, incidence, and risk factors and indicators for peri-implant diseases (AO/AAP systematic review and meta-analysis), J Periodontol
- Mahardawi et al. 2023, The lack of keratinized mucosa as a risk factor for peri-implantitis: a systematic review and meta-analysis, Sci Rep
- Berglundh et al. 2018, Peri-implant diseases and conditions: Consensus report (2017 World Workshop)
- Renvert et al. 2018, Peri-implant health, peri-implant mucositis, and peri-implantitis: case definitions
- Schwarz et al. 2018, Peri-implantitis
- Herrera et al. 2023, EFP S3 clinical practice guideline on peri-implant diseases
- Derks & Tomasi 2015, Peri-implant health and disease: a systematic review of prevalence
- Lee et al. 2017, Prevalences of peri-implant mucositis and peri-implantitis
- Diaz et al. 2022, Prevalence of peri-implant diseases
- Wilensky et al. 2023, Surgical decontamination in peri-implantitis
- Hart et al. 2024, Decontamination methods in peri-implantitis therapy
- Monje et al. 2016, Maintenance therapy interval and peri-implant disease
- Monje et al. 2025, Outcomes of surgical peri-implantitis therapy (Periodontology 2000; DOI 10.1111/prd.12643)
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
Immediate Implant Placement: A Protocol for Case Selection and Predictable Results
Next
Sinus Lift in Implant Dentistry: Lateral Window or Transcrestal Approach?