Guided Bone Regeneration: A Clinical Guide to Every Bone Defect
Guided bone regeneration works when the defect is diagnosed correctly, the membrane protects the space, and the flap closes without tension.

Table of Contents
Related clinical guides
I still think the most useful way to teach guided bone regeneration is not to begin with a product catalog. It is to begin with a race.
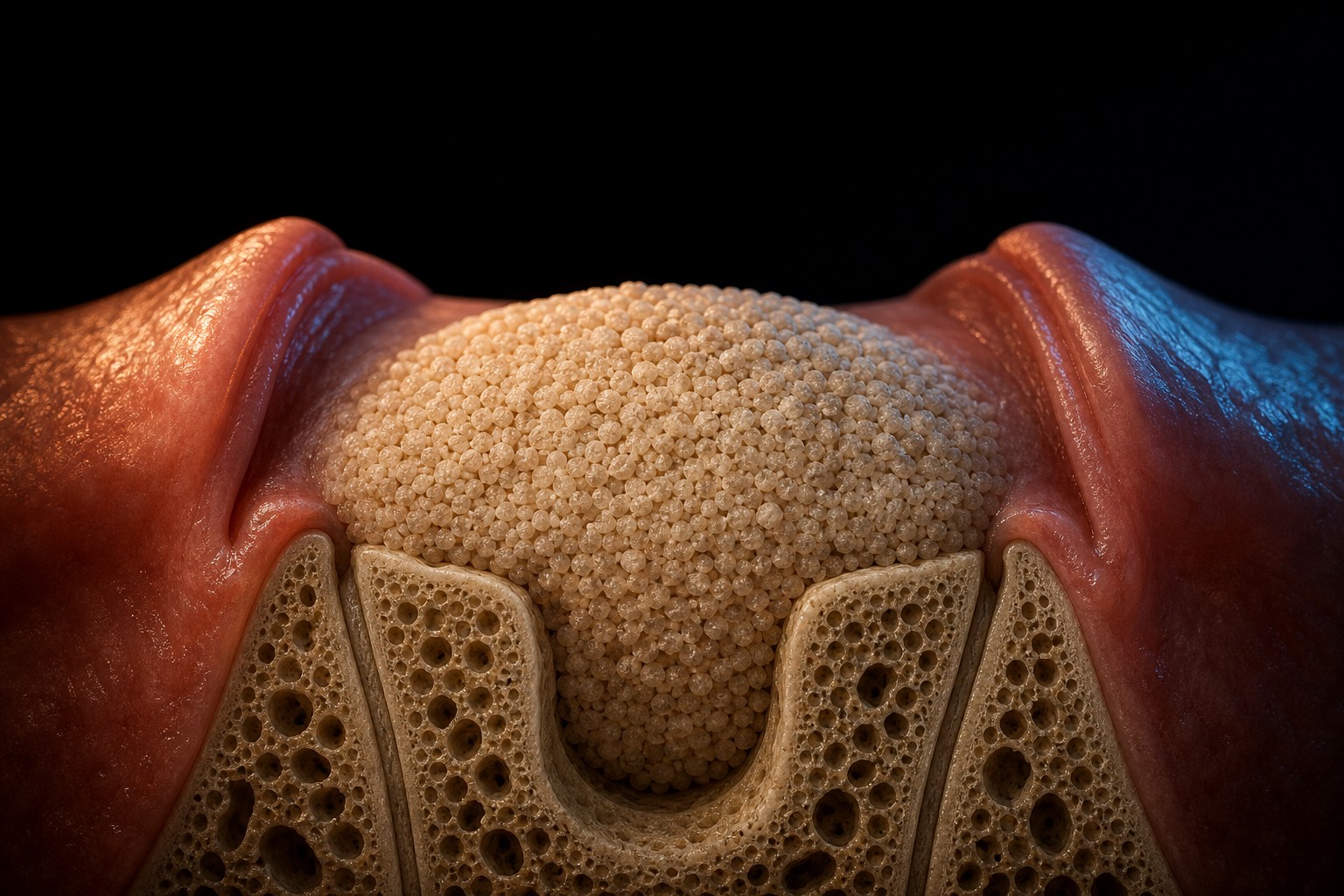
Soft tissue moves fast. Bone moves slowly. If both tissues are allowed to enter the same defect at the same time, soft tissue usually wins. The membrane is how we change the rules of the race.
That is the simple idea behind GBR, but simple does not mean easy. In real surgery the problem is never just "place graft and membrane." It is deciding whether the defect can hold space, whether the flap can close passively, whether the implant can be placed in the correct prosthetic position, and whether the patient can keep the wound quiet while biology does its work. That changes everything about how the case is planned.
Guided Bone Regeneration In Implant Dentistry: Principles, Membranes, And Bone Grafting Techniques
In clinical practice, guided bone regeneration in implant dentistry is not the same question as choosing a bone graft. The real decision is anatomical: what defect is present, how much space must be maintained, which membrane can protect that space, and whether closure can be achieved without tension? GBR vs bone graft is not a semantic detail. A bone graft is the material that helps fill or support the defect. Guided bone regeneration is the surgical system around that material: recipient-bed preparation, angiogenesis, membrane selection, space maintenance, fixation, flap release, and wound stability. The International Team for Implantology also emphasizes that bone augmentation can compensate for post-extraction ridge modeling when immediate or early implant placement is correctly selected (ITI consensus on post-extraction sites).
When I choose a guided bone regeneration membrane, I am not asking only whether it resorbs. I am asking whether the membrane can protect the clot and maintain the space for the defect in front of me. A collagen membrane may be enough for a contained contour defect. A reinforced non-resorbable membrane may be needed when the defect cannot maintain its own shape.
What GBR Actually Does
GBR uses a barrier membrane to exclude epithelial and connective-tissue cells from a bone defect. Under that membrane, the graft helps maintain volume and supports clot stability while bone cells arrive from the surrounding walls and blood supply. This membrane principle has been part of implant regeneration for decades, and it remains the logic behind most ridge augmentation procedures today, as summarized in the narrative review by Hämmerle and Karring, 1998.
So when a clinician says "I did a bone graft," I always want to know one more thing: what was the defect morphology?
A contained socket is a very different problem from a buccal dehiscence, a horizontal ridge defect from a vertical one, and a peri-implant gap in an immediate implant from a knife-edge ridge with no facial wall. The material matters. The morphology matters more.
The PASS Checklist I Use Before Opening A Membrane
Wang and Boyapati described the PASS principles for predictable bone regeneration: primary closure, angiogenesis, space maintenance, and stability Wang and Boyapati, 2006. I like the acronym because it prevents us from hiding behind biomaterials.
| PASS principle | Chairside translation | What usually goes wrong |
|---|---|---|
| Primary closure | The flap closes passively over the graft | You pull the flap to make it meet, then the membrane exposes |
| Angiogenesis | The site has enough blood supply | Over-deperiostealized flaps, poor recipient bed, smoking, infection |
| Space maintenance | The defect volume is held open | A collagen membrane collapses into a large non-contained defect |
| Stability | The clot, graft, membrane, and implant do not move | Mobile graft particles, loose membrane, unstable implant, weak sutures |
If one part fails, the biology becomes less forgiving. This is why I prefer to plan the flap and closure before I fall in love with the graft.
Defect Classification: The Case Tells You The Technique
Surgical video: classification should change the surgery.
This is where GBR becomes practical. The defect classification is not a label for the article; it should change implant timing, membrane support, flap design, and closure strategy.
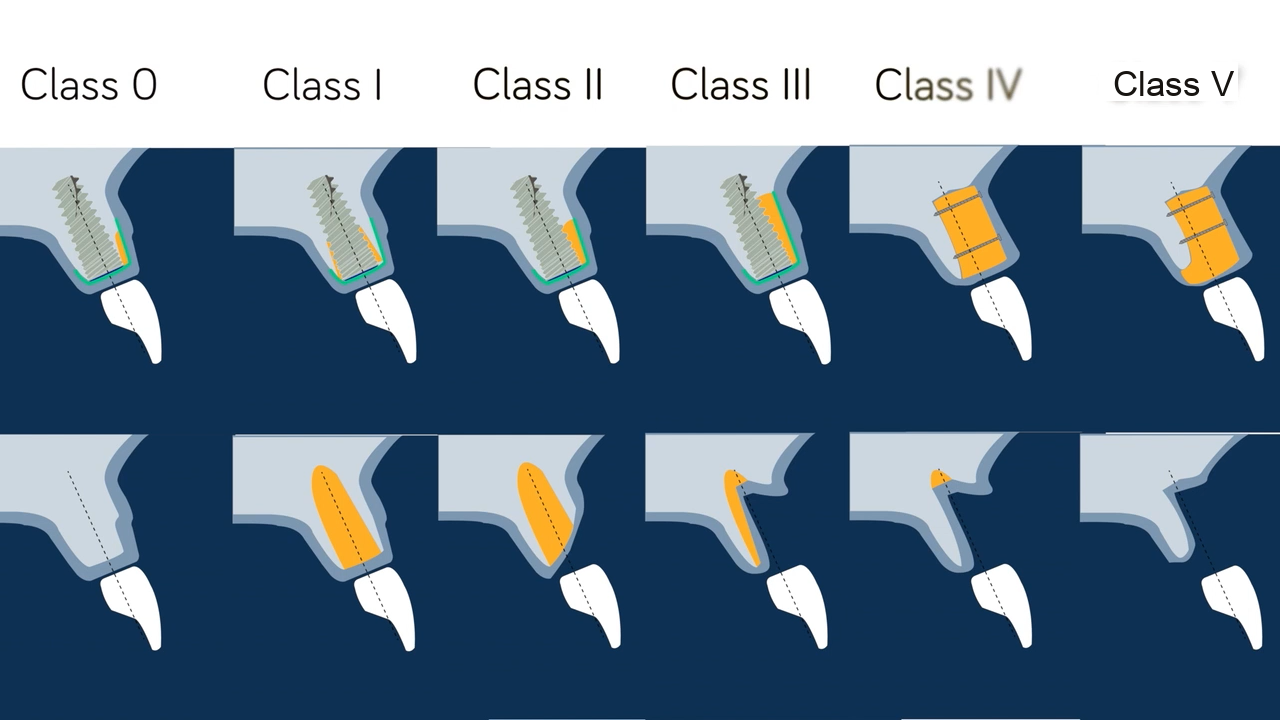
The framework I keep returning to is the horizontal-defect classification described by Benic and Hammerle (Benic and Hammerle, 2014). They organize the bony envelope around the planned implant into classes, and each class quietly tells you how much the membrane and graft will have to do. Here is how I read that scheme at the chair, faithful to the original definitions.
- Class 0: the implant can be placed in the correct prosthetic position inside an intact bony envelope, yet a contour augmentation is still indicated to rebuild the buccal profile and the soft-tissue support over it. This is the class people most often under-treat, because the implant feels stable and they assume no graft is needed.
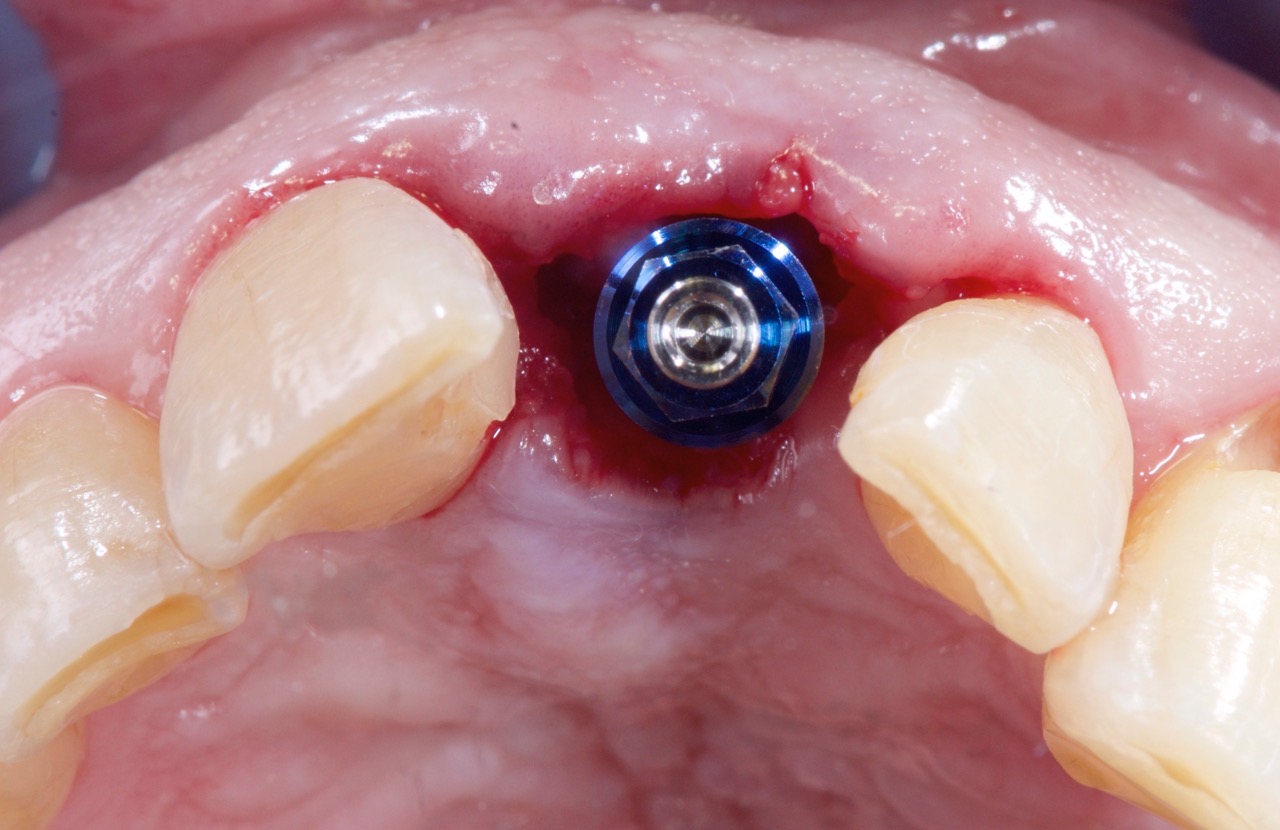
- Class 1: a gap between the implant surface and the intact surrounding bone walls, the situation you most often meet at immediate placement into a fresh socket. The bony housing is still there, so the walls do much of the space-maintenance work and the gap fills predictably once it is grafted and protected.
- Class 2: a defect restricted to the buccal or lingual aspect with the mesial and distal walls intact. It is still partly contained, but the missing facial wall means the membrane has to define the contour the bone no longer provides.
- Class 3: a true dehiscence where the adjacent walls no longer maintain volume on their own. Space maintenance now depends on graft choice, membrane support, and fixation rather than on residual anatomy.
- Class 4: a horizontal ridge deficiency where width is the limiting factor and the implant cannot be placed in the ideal position without first rebuilding the buccal plate.
- Class 5: vertical or combined horizontal-and-vertical defects, the cases that punish optimism. Here the membrane must hold a space the anatomy fights to collapse, and staging is usually the disciplined choice.
I follow the published class definitions here rather than my own buckets, because the value of the scheme is that it maps each defect to a predictable amount of membrane support and fixation. My one personal caveat: do not graft because a protocol or the calendar tells you to. Graft because the defect class in front of you genuinely needs volume or contour.
From Defect Class To Membrane Support And Fixation
The reason I spend so long on classification is that the class is really a prescription for how hard the membrane and fixation have to work. A contained Class 1 defect is forgiving: the residual walls hold the graft and do much of the space-maintenance work, so a single resorbable collagen membrane is often enough, sometimes without fixation pins at all.
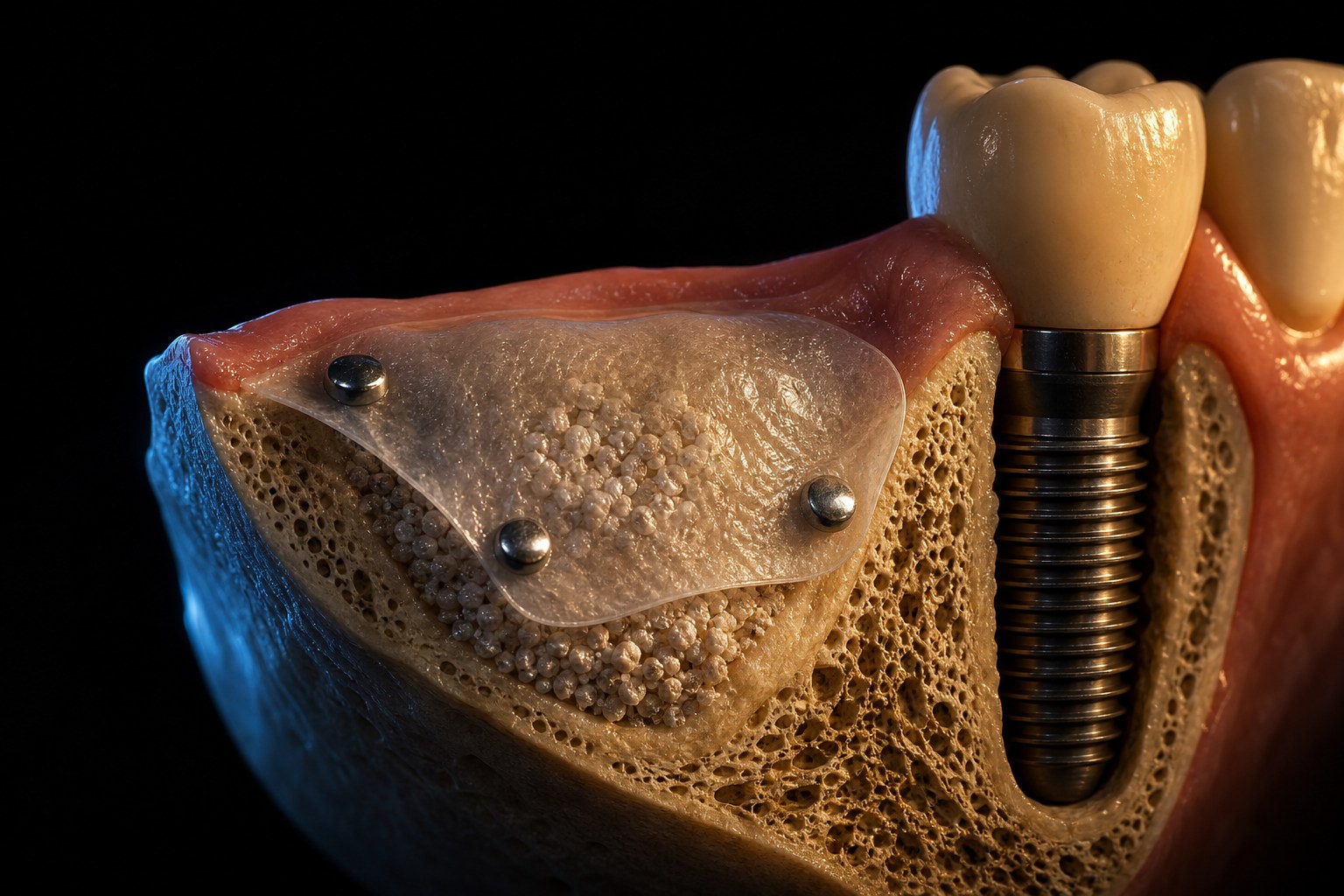
Class 2 and Class 3 change that calculus. Once the buccal wall is gone, the membrane stops being a passive barrier and starts defining the contour the bone no longer provides. Here I become more deliberate: a slow-resorbing particulate graft helps the membrane hold its shape, and I frequently tack the membrane with a buccal fixation pin so it cannot migrate during closure. A membrane that slides even a millimeter can leave a graft particle uncovered, and an uncovered particle is a future exposure waiting to happen.
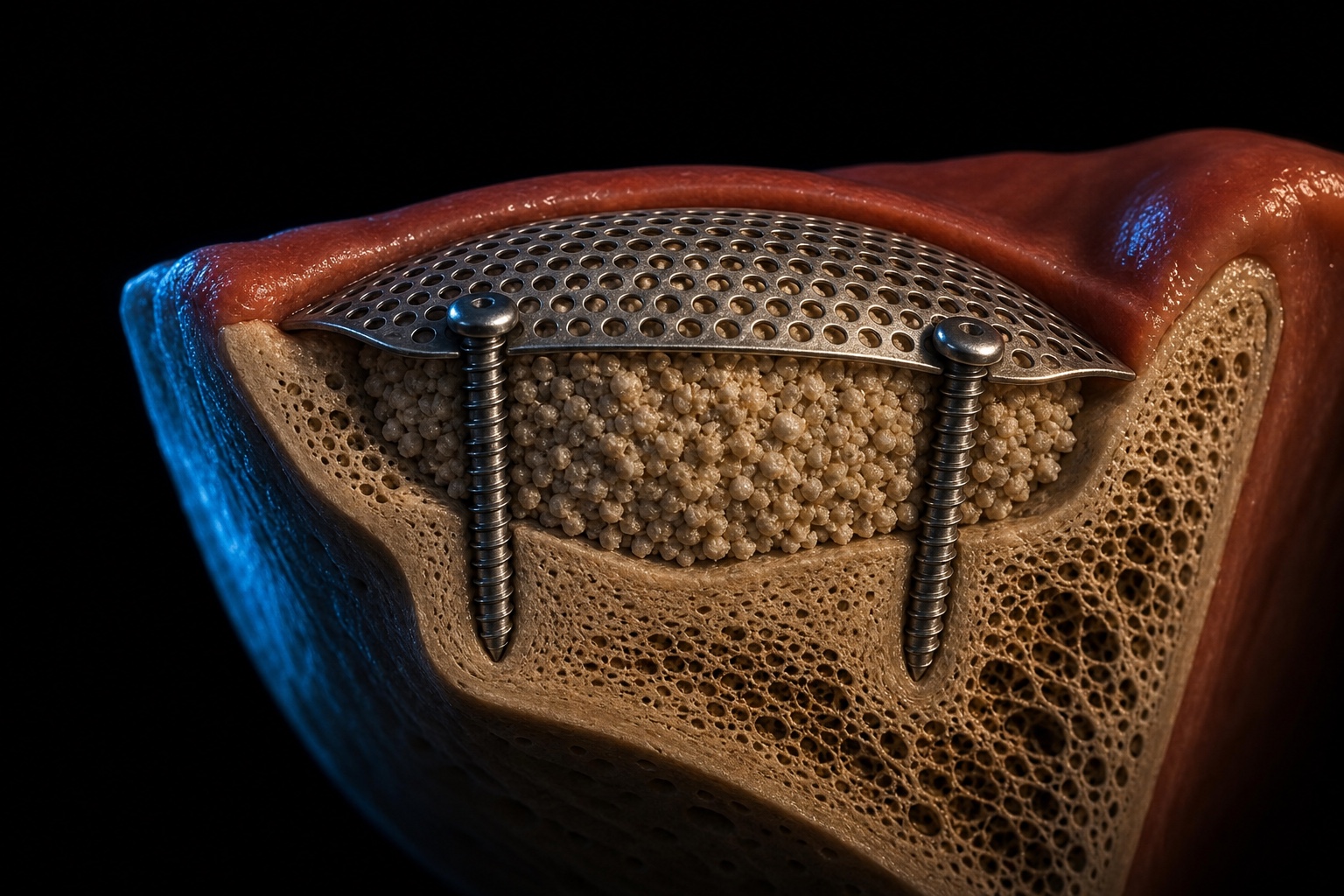
Class 4 and Class 5 defects are where the membrane genuinely becomes the architecture. In a horizontal Class 4 case, the goal is to recreate a buccal plate that is not there, so the membrane has to maintain a space against the constant inward pressure of the flap and the lip. I plan for rigid space maintenance from the start: a dense slow-resorbing graft, a reinforced or titanium-supported membrane, or tenting screws holding the membrane off the residual ridge. Fixation is not optional here.
Class 5 vertical and combined defects punish optimism. The membrane must hold a space the anatomy actively fights to collapse, the blood supply has further to travel, and the soft tissue has the least give. For these I default to staging and meticulous fixation, and I accept that recognizing a genuine Class 5, one that belongs in experienced hands, is itself a clinical skill.
Surgical video: buccal contour support is a hard-tissue diagnosis.
This video belongs in GBR, not the CTG section. If the facial contour is deficient and lip support depends on ridge volume, the plan is membrane, graft stability, and prosthetic contour. Soft tissue can refine the envelope, but it does not replace missing buccal hard-tissue volume. When a graft is the right adjunct to thicken the overlying tissue after the bone is rebuilt, I compare the harvesting options in four connective tissue harvesting techniques.
The more contained the defect, the more the defect itself helps you. The less contained the defect, the more the surgeon must create and protect the missing walls. If you want a defect-by-defect walkthrough of how each of these morphologies is actually rebuilt, I cover them in how to solve the most common bone defects with GBR.
That is where the membrane stops being an accessory and becomes the architecture.
Graft Materials: Do Not Ask The Wrong Question
The wrong question is: "Which graft is best?"
The better question is: "What do I need this material to do for this defect?"
| Material group | Main clinical advantage | Limitation |
|---|---|---|
| Autogenous bone | Living cells and strong biology | Donor morbidity and faster remodeling |
| Allograft | Human bone matrix without a second surgical site | Variable remodeling profile depending on processing |
| Xenograft | Slow resorption and strong volume maintenance | Less biological activity than autogenous bone |
| Synthetic graft | Controlled composition and no donor tissue | Performance depends heavily on formulation and indication |
For many contour and horizontal defects, I like slow-resorbing particles because they help maintain the ridge envelope. For biologically demanding sites, I may mix autogenous chips with a slower-resorbing scaffold. But I do not pretend the mixture saves a poorly closed flap.
Flap Design, Graft Handling, And Membrane Adaptation
Before any graft goes into the defect, the case is usually won or lost in flap design and recipient-bed preparation. I raise a full-thickness flap with enough extension for tension-free advancement, keeping releasing incisions disciplined: too timid and the flap will not advance, too aggressive and I compromise the blood supply the graft depends on. Vertical releasing incisions sit at line angles, never over the graft. The periosteum is what lets a flap stretch, so a controlled periosteal release at the base of the buccal flap converts a flap that closes under tension into one that drapes passively over the augmented site.
Recipient-bed preparation matters more than most courses admit. Dense, avascular cortical bone contributes no cells or blood, so I perforate the cortex with a small round bur to open marrow spaces and connect the graft to a living blood supply rather than leaving it on an inert wall.
Graft handling is similarly decisive. I hydrate particulate graft in sterile saline or the patient's blood, place it without overpacking, and shape it to the contour I want; overpacking crowds out the clot the graft needs to organize. For stronger biology I mix autogenous chips with a slower-resorbing scaffold, so the autogenous fraction drives healing while the scaffold holds volume.
The membrane is then adapted to extend past the bony margins on every side and lie flat against sound bone, not graft. A membrane that ends at the defect edge will roll, expose graft, and invite contamination, so where the defect is non-contained I fix the membrane before I close: a membrane that moves during suturing has already failed.
Membrane Choice: Collagen Is Not A Religion


Collagen membranes are convenient, resorbable, and useful in many everyday GBR procedures, and forgiving because they need no removal surgery. But they are not magic. In large non-contained defects, a soft membrane collapses into the defect unless the graft, pins, screws, or anatomy maintain the space.
A reinforced non-resorbable membrane can be the right tool when the defect needs a tent. The tradeoff is exposure risk and a second intervention, and that tradeoff changes the whole case design.
Simultaneous Or Staged GBR?
Surgical video: socket preservation is not just filling a hole.
The socket itself tells you which decision you are really making. A socket with intact walls is a volume-preservation problem, where graft and membrane simply protect what is there. A socket with a missing or fractured buccal wall is a reconstruction problem, where you rebuild a wall before you can trust the contour. A heavily compromised socket is often a timing problem, where the honest move is to graft, let the site heal, and postpone implant placement. When the decision is to preserve volume at extraction, the illustrated workflow lives in my alveolar ridge preservation guide.
This is the decision I want dentists to slow down on.
| Situation | My default direction | Why |
|---|---|---|
| Implant can be placed in ideal 3D position with primary stability | Simultaneous GBR can be reasonable | The implant position is not compromised by the defect |
| Implant position would be dictated by remaining bone | Stage the augmentation | The prosthetic plan should drive implant position, not the defect |
| Large vertical or combined defect | Usually staged | Space maintenance and closure are more demanding |
| Thin buccal contour defect with stable implant | Simultaneous contour augmentation | The goal is envelope stability, not heroic reconstruction |
| Active infection or unstable soft tissue | Delay and control the site | Regeneration does not rescue uncontrolled inflammation |
The staged approach is not failure. It is sometimes the most disciplined decision in the room.
The Closure Is The Case
You can choose the right graft and the right membrane and still lose the procedure at the suture line. Tension-free closure is not cosmetic; it is part of the biology.
I release the flap until it covers the graft passively. If the flap only closes because I am pulling it, I assume the wound will punish me later. The sutures should maintain the decision, not force it. If your closure repertoire stops at interrupted sutures, this is the highest-yield place to expand it: I walk through my go-to options in three suturing techniques for GBR you can start using tomorrow.
Surgical video: the closure is part of the regeneration.
Most GBR failures I am asked to review are not material failures. They are stability, flap, exposure, and closure failures. The graft and the membrane usually did their part; the wound was simply not kept quiet and sealed long enough for the biology to finish. That is why I treat suturing as a regenerative step, not a finishing touch.
When Things Go Wrong: Exposure And Complication Management
The most common complication in GBR is membrane exposure, and how you manage it depends on which membrane you used and how early it happens. A small, late exposure of a resorbable collagen membrane in an otherwise quiet site can often be managed conservatively: reinforce hygiene, add a chlorhexidine regimen, watch closely, and let the membrane resorb while the graft organizes. A resorbable membrane that exposes is not automatically a lost case.
A reinforced non-resorbable membrane that exposes is more urgent. Because it does not resorb, exposed material becomes a nidus for bacterial colonization, and a contaminated membrane over a graft is a setup for infection and graft loss. My threshold for early removal is low: I would rather remove the membrane and salvage part of the augmentation than chase a heroic result and lose the whole site. That asymmetry is why I weigh exposure risk so heavily when I choose the membrane.
Other complications follow the same principles in reverse. Graft mobility traces back to inadequate fixation or overpacking. Flap dehiscence traces back to closure under tension, which is why passive closure stays non-negotiable. Infection demands control before regeneration can be reconsidered, because no membrane rescues an uncontrolled infection. The pattern is consistent: the material is rarely the villain. Stability, blood supply, space maintenance, and closure decide whether a GBR case heals, and each is under the surgeon's control long before the membrane is opened.
What This Guide Does Not Solve
GBR does not compensate for poor implant position. It does not make an infected site clean. It does not turn a mobile provisional into a good idea. And it does not remove the need for maintenance, smoking control, patient compliance, and honest case selection.
The beautiful part of GBR is that it is biological. The frustrating part is also that it is biological.
Case selection is the quiet skill that separates predictable operators from frustrated ones. A smoker with poor compliance and a large vertical defect is not the patient for your first vertical augmentation. A patient with active periodontal disease needs that disease controlled first, because the same bacteria that destroyed the bone will not respect a membrane. And a patient who will not keep the wound undisturbed during healing has, in effect, already opted out of the most demanding part of the protocol.
The clinicians who get consistent GBR results are not the ones with the most expensive membranes. They diagnose the defect accurately, respect the four PASS principles, choose the membrane and graft for the case rather than the habit, and refuse to compromise on closure.
Go Deeper Inside The Interactive GBR Ebook
This public article is the map. The surgical videos, defect-by-defect protocols, suturing sequences, and quizzes live inside the interactive Guided Bone Regeneration ebook. It includes the full workflow for bone dynamics after extraction, socket preservation, osseointegration, membrane handling, and GBR suturing.
If you are planning your first serious GBR case, do not start by buying a different membrane. Start by learning to read the defect.
References
- Wang and Boyapati, 2006
- Hämmerle CHF, Karring T. Guided bone regeneration at oral implant sites. Periodontol 2000. 1998;17:151-175 (narrative review; PMID 10337322)
- Benic GI, Hammerle CHF. Horizontal bone augmentation by means of guided bone regeneration. Periodontol 2000. 2014;66(1):13-40 (PMID 25123759)
- ITI consensus on implants in post-extraction sites
Frequently Asked Questions
What is guided bone regeneration?
Guided bone regeneration is an implant surgery technique that uses a barrier membrane, usually with a graft material, to protect a bone defect from fast-growing soft tissue while bone-forming cells repopulate the space.
What are the PASS principles in GBR?
PASS stands for primary wound closure, angiogenesis, space maintenance, and stability. It is a practical checklist for predictable bone regeneration.
When should GBR be staged instead of simultaneous with implant placement?
Staging is safer when the defect prevents ideal implant position, primary stability, or tension-free closure. Simultaneous GBR is more suitable when the implant can still be placed prosthetically and stabilized correctly.
Which membrane is best for GBR?
There is no universal membrane. Resorbable collagen membranes are useful in many moderate defects; reinforced non-resorbable membranes can support larger horizontal or vertical defects but demand stricter soft-tissue management.
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
The Connective Tissue Graft: Harvesting Techniques, Indications, and CTG vs FGG
Next
Immediate Implant Placement: A Protocol for Case Selection and Predictable Results
Related Articles
How to Solve the Most Common Bone Defects With Guided Bone Regeneration
13 min read
3 Suturing Techniques For Guided Bone Regeneration That You Can Start Using Tomorrow
12 min read